There has been an explosion in sports participation, especially for women, in the last 35 years mainly because of Title IX. In 2005–2006, nearly 3 million girls and 4.2 million boys participated in high school athletics, and many more participated in club sports and recreational activities. On the other end of the spectrum, the prevalence of obesity in the United States is at an all-time high. Proper nutrition in combination with the appropriate amount of physical activity is of paramount importance for this era of adolescents.
There has been an explosion in sports participation, especially for women, in the last 35 years mainly because of Title IX. In 2005–2006, nearly 3 million girls and 4.2 million boys participated in high school athletics, and many more participated in club sports and recreational activities. On the other end of the spectrum, the prevalence of obesity in the United States is at an all-time high. Proper nutrition in combination with the appropriate amount of physical activity is of paramount importance for this era of adolescents.
Growth
Boys and girls typically follow specific patterns of growth from infancy to adulthood. Infancy and early childhood are characterized by a period of rapid growth. Middle childhood is typically a period of small, constant gains. Adolescence is again characterized by rapid growth, and then growth is relatively slow and constant until adulthood. School-aged children and adolescents are at a critical time period because nutritional deficiencies could have a significant effect not only on growth and development but also on athletic and academic performance. Before puberty, there is no significant difference between boys and girls in regards to biomechanics, body composition, or nutritional requirements.
It is challenging to make general recommendations for nutritional needs for adolescents because not only age but also stage of physical maturity and level of physical activity must be considered. The dietary reference intakes, which include the recommended dietary allowances (RDA), adequate intakes (AI), and tolerable upper intakes levels for adolescents, are stated for three age groups, as shown in Table 1 .
| Weight a | Height a | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (y) | (kg) | (lb) | (cm) | (in) | Vitamin A (μg RE) b | Vitamin D (μg) c | Vitamin E (mg α-TE) d | Vitamin K (μg) | Vitamin C (mg) | Iron (mg) | Zinc (mg) | Iodine (μg) | Selenium (μg) | |
| Children | 4–6 | 20 | 44 | 112 | 44 | 500 | 10 | 7 | 20 | 45 | 10 | 10 | 90 | 20 |
| 7–10 | 28 | 62 | 132 | 52 | 700 | 10 | 7 | 30 | 45 | 10 | 10 | 120 | 30 | |
| Males | 11–14 | 45 | 99 | 157 | 62 | 1000 | 10 | 10 | 45 | 50 | 12 | 15 | 150 | 40 |
| 15–18 | 66 | 145 | 176 | 69 | 1000 | 10 | 10 | 65 | 60 | 12 | 15 | 150 | 50 | |
| 19–24 | 72 | 160 | 177 | 70 | 1000 | 10 | 10 | 70 | 60 | 10 | 15 | 150 | 70 | |
| 25–50 | 79 | 174 | 176 | 70 | 1000 | 5 | 10 | 80 | 60 | 10 | 15 | 150 | 70 | |
| Females | 11–14 | 46 | 101 | 157 | 62 | 800 | 10 | 8 | 45 | 50 | 15 | 12 | 150 | 45 |
| 15–18 | 55 | 120 | 163 | 64 | 800 | 10 | 8 | 55 | 60 | 15 | 12 | 150 | 50 | |
| 19–24 | 58 | 128 | 164 | 65 | 800 | 10 | 8 | 60 | 60 | 15 | 12 | 150 | 55 | |
| 25–50 | 63 | 138 | 163 | 64 | 800 | 5 | 8 | 65 | 60 | 15 | 12 | 150 | 55 | |
a Weights and heights of reference adults are actual medians for the US population of the designated age, as reported by National Health and Nutrition Examination Survey II. The use of these figures does not imply that the height-to-weight ratios are ideal.
b Retinol equivalents: 1 retinol equivalent = 1 μg retinol or 6 μg β-carotene.
c As cholecalciferol: 10 μg cholecalciferol = 400 IU of vitamin D.
d α-Tocopherol equivalents: 1 mg d-α tocopherol = 1 α-TE. See text for variation in allowances and calculation of vitamin E activity of the diet as α-tocopherol equivalents.
Caloric needs for adolescents vary considerably depending on age, growth rate, and level of physical maturity. The RDA for caloric and protein needs for male and female individuals aged 11 to 24 are shown in Table 2 . Calories per unit height (cm) and weight (kg) can be used for general estimates. However, this does not reflect energy expenditure from exercise or growth rate.
| Weight | Height | Energy | Protein | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (y) | (kg) | (lb) | (cm) | (in) | Kcal/d | Kcal/kg | g/d | g/kg a | |
| Children | 4–6 | 20 | 44 | 112 | 44 | 1800 | 90 | 24 | 1.1 |
| 7–10 | 28 | 62 | 132 | 52 | 2000 | 70 | 28 | 1.0 | |
| Males | 11–14 | 45 | 99 | 157 | 62 | 2500 | 55 | 45 | 1.0 |
| 15–18 | 66 | 145 | 176 | 69 | 3000 | 45 | 59 | 0.9 | |
| 19–24 | 72 | 160 | 177 | 70 | 2900 | 40 | 58 | 0.8 | |
| 25–50 | 79 | 174 | 176 | 70 | 2900 | 37 | 63 | 0.8 | |
| Females | 11–14 | 46 | 101 | 157 | 62 | 2200 | 47 | 46 | 1.0 |
| 15–18 | 55 | 120 | 163 | 64 | 2200 | 40 | 44 | 0.8 | |
| 19–24 | 58 | 128 | 164 | 65 | 2200 | 38 | 46 | 0.8 | |
| 25–50 | 63 | 138 | 163 | 64 | 2200 | 36 | 80 | 0.8 | |
a Amino acid score of typical United States diet is 100 for all age groups, except young infants. Digestibility is equal to reference proteins. Values have been rounded upward to 0.1 g/kg.
The role of carbohydrates, proteins, and fats in athletic performance
Basic nutrition is vital for aiding in growth, providing energy, and achieving good health and school performance. Sports nutrition expands on these basic principles to enhance athletic performance by reducing fatigue and susceptibility to disease and injury while concurrently allowing an athlete to train harder and longer and recover faster . The underlying macronutrients that fuel physical activity are carbohydrates, proteins, and fats. It is crucial for athletes to take in equal or more calories than they are expending to prevent an energy deficit, which can result in loss of muscle mass, menstrual dysfunction, loss of or failure to gain bone density, and increased risk for fatigue, injury, or illness .
In order for any muscle to do work, adenosine triphosphate (ATP) is required; it also must be replenished continuously during physical activity in order for the activity to continue . When energy demands increase during exercise, the body relies on three different systems to transfer stored energy to ATP: the phosphagen, glycolytic, and aerobic systems . The phosphagen system uses stored phosphocreatine in muscle cells to directly produce ATP and is used primarily for short-term, high-intensity exercise, such as sprinting, high jumping, or a rapid weight lift. Myocytes can only store small amounts of phosphocreatine, however, and ATP production is limited accordingly. This system can only deliver enough ATP to support activity that lasts less than 20 seconds. The glycolytic system is also a short-term fuel provider and supplies ATP for intense activity that lasts from 20 to 45 seconds . Both of these systems are anaerobic, whereas the third system, oxidative phosphorylation, requires oxygen to produce ATP through the oxidation of carbohydrates, fats, and proteins. This system is used for activity lasting longer than 45 seconds .
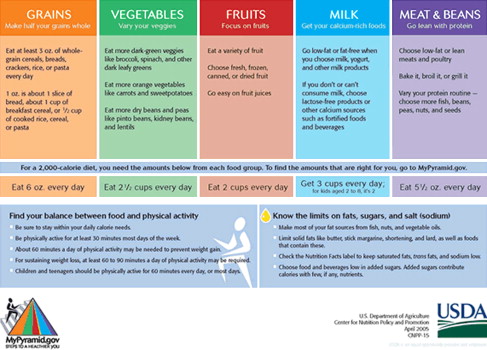
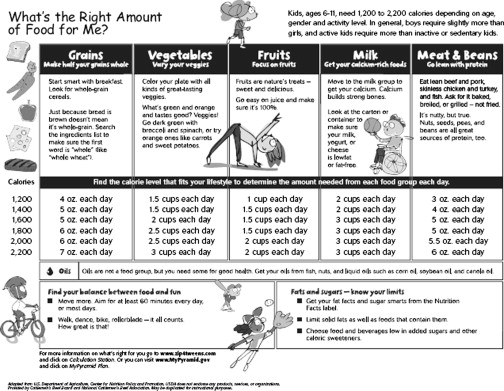
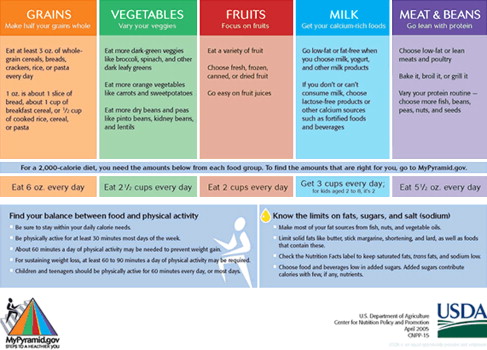
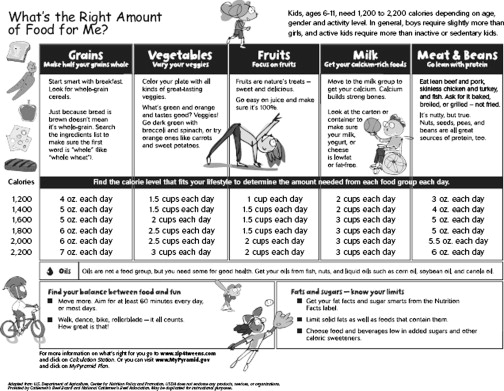
In 2005, the government introduced a revision of their food guidance system. Originally, it was developed in 1992 as the food pyramid guide (FPG). “MyPyramid,” released in 2005, symbolizes a personalized approach to healthy eating and physical activity ( Figs. 1 and 2 ). It is recommended for everyone to obtain at least the lower end of the recommended range of servings, whereas the higher end is suggested for athletes who expend a significant amount of energy in physical activity. The Institutes of Medicine Food and Nutrition Board recently revised caloric recommendations as follows :
Male athletes aged 30 years and older
Total energy expenditure = 662 − 9.53 × age (years) + 1.48 [physical activity] × (15.91 × weight [kg] + 539.6 × height [m])
Female athletes aged 30 years and older
Total energy expenditure = 354 − 6.91 × age (years) + 1.45 [physical activity] × (9.36 × weight [kg] + 726 × height [m])
For male and female athletes between 19 and 30 years
Add 7 kcal/d for women and 10 kcal/d for men for every year before 30
For children and teens younger than 19 years
Boys/girls aged 7 to 10: 2000 calories/d
High school boys: 3000 to 6000 calories/d
High school girls: 2200 to 4000 calories/d
Carbohydrates are the primary source of fuel during exercise and contain approximately 4 kcal/g. An adult athlete’s diet should typically be made up of 60% to 65% carbohydrates, whereas an adolescent athlete’s diet should contain 55% to 60% . In 2002, the Institute of Medicine established the RDA of carbohydrates for adults and children as 130 g/d, which is based on the amount needed to supply the brain with adequate glucose . Beyond this specific RDA, they also set for carbohydrates an acceptable macronutrient distribution range of 45% to 65% of total caloric intake. Both of these guidelines are intended to meet the needs of 95% of the general population .
Carbohydrates taken in through food are necessary to maintain blood glucose and is stored as glycogen in the muscles and liver . Muscle glycogen is the fastest form of energy available to the working muscle and can be released up to three times quicker than energy from any other source . Muscle glycogen and blood glucose are also the limiting factors in any type of human performance . As exercise intensity increases, the more muscle glycogen is relied on as an energy source ; however, as the duration of exercise increases, the source of energy shifts from muscle glycogen to circulating blood glucose . During long periods of exercise, muscle glycogen and blood glucose levels both become low, and unless carbohydrates are replenished, an athlete will not be able to perform at a high level . A study by Ahlborg and colleagues found that work time to exhaustion was directly related to the quantity of initial glycogen stores in the working muscles. They showed that by manipulating the quantity of carbohydrate in the diet, the concentration of glycogen in the muscle could be altered, as could the athlete’s time to exhaustion.
Endurance athletes who train aerobically for more than 90 minutes daily need approximately 6 to 10 g of carbohydrate/kg of body weight/day to restore glycogen levels during training. This amounts to roughly 300 to 700 g of carbohydrate . Carbohydrate ingestion during exercise that lasts longer than 1 hour also may help increase endurance . Athletes can help maintain their body’s supply of energy by consuming approximately 25 to 30 g of carbohydrate every half hour during exercise. This practice can improve performance by maintaining blood glucose levels after muscle glycogen has been diminished, because 1 g carbohydrate/min is delivered to the tissues as fatigue sets in .
Proteins carry out many bodily functions and aid in the structure of skin, hair, nails, and muscle. Protein normally provides less than 5% of the energy expended at rest and during mild exercise . However, as exercise duration increases, proteins contribute to the maintenance of blood glucose via gluconeogenesis in the liver . Proteins contain approximately 4 kcal/g, similar to carbohydrates, and the current RDA for protein is 0.8 g/kg body weight/day for the general population.
Athletes may require a higher protein intake in the early stages of resistance and endurance training because of increasing muscle mass . In the beginning of training, the recommended protein intake is 1.5 to 1.7 g/kg body weight/day. As training enters the maintenance phase, protein intake may be decreased to 1.0 to 1.4 g/kg body weight/day. Protein requirements are necessarily greater in adolescents than in sedentary adults because of growth and development of lean body mass. The RDA of protein for active children and adolescents is 2 g/kg/d . Overall, the protein recommendation for active adults and children is 12% to15% of energy intake . Resistance training may require a higher protein intake, and weight lifters consume anywhere from 1.2 to 3.4 g/kg body weight/day . Bodily protein synthesis seems to be at a maximum in strength-training athletes who consume 1.4 g protein/kg body weight/day .
Consuming more protein than the body can use is unnecessary and should be avoided. This is an important guideline to remember as ergogenic aids and other supplements become increasingly popular in modern society. When athletes consume diets that are high in protein, they compromise their carbohydrate status, which may affect their ability to train and compete at peak levels. Taking large amounts of protein or amino acid supplements can also lead to dehydration, urinary loss of calcium, weight gain, and stress on the kidneys and liver because protein requires almost seven times more water for metabolism than fat or carbohydrates .
Fats are used as a secondary fuel source after carbohydrates. Fats provide necessary vitamins, are essential for menstrual function, and protect the internal organs. They contain 9 kcal/g and should make up 20% to 25% of an athlete’s diet. There is no specific RDA for fat intake, but it is recommended that athletes consume no more than is recommended for a sedentary person. Children and adults should take in no more than 10% saturated, 10% polyunsaturated, and 10% monounsaturated fats in their diet.
Fat is the major fuel for light- to moderate-intensity exercise (<60% VO 2max ). During low-intensity exercise that lasts longer than 30 minutes, there is a gradual shift away from carbohydrate metabolism with an increasing reliance on fat metabolism, or beta-oxidation, as the primary energy source . With training, the quantity of mitochondrial enzymes can increase, which in turn increases fatty acid oxidation. Glucose uptake, glycolysis, and glycogenolysis are then increasingly inhibited by free fatty acid oxidation within the skeletal muscle . Trained individuals are able to use fat stores more efficiently than untrained athletes, who rely more heavily on carbohydrate stores.
One aspect of performance unique to women and younger adolescents is their higher capacity for lipid oxidation . Women are believed to oxidize fat better than men because of fluctuating hormones in the menstrual cycle. These hormones dramatically influence substrate selection and most likely account for the reduced reliance on carbohydrates . Children and adolescents generally have higher levels of glycerol in their blood, which results in increased use of free fatty acids during exercise. Despite their increased lipid use, it is still recommended that an adolescent’s consumption of fats be no more than 30% of their daily caloric intake .
It is important for physically active children and adolescents to consume enough nutrients to meet their needs for growth, tissue maintenance, and physical and intellectual performance . It is difficult to establish specific recommended intakes, however, because of large individual variability. During growth spurts, adolescents should consume an additional 500 kcal/d above their usual intake . Carbohydrates do not seem to play as great a role for youth in exercise as for adults because of the submaximal glycolytic capacity characteristic of younger age . The RDA for carbohydrates in children and adolescents is at least 50% of total daily caloric intake. The children’s FPG (see Fig. 2 ) is a useful tool for ensuring adequate nutrition in the diet. It is important to remember that active children should consume the high end of the range of recommended servings for each food group.
Precompetition meals are essential for athletes to maintain energy levels for the exercising muscles during competition . In a study by Sherman and colleagues, cycling performance was improved by 15% when athletes consumed 4.5 g/kg body weight carbohydrate 4 hours before moderate-intensity exercise. Consuming 1 to 4.5 g of carbohydrate/kg body weight 1 to 4 hours before activity helps to maintain blood glucose levels during exercise and ensure adequate carbohydrate availability . It is not recommended for athletes to fast before competition because of the risk of their blood glucose levels decreasing during exercise and impairing performance .
A study by Thomas and colleagues also showed that the glycemic index of an individual’s food intake may affect performance. Cyclists who consumed low glycemic index carbohydrates (<60) 1 hour before pedaling to exhaustion had a significantly longer endurance time than individuals who consumed medium (60–80) and high glycemic foods (>80). High glycemic foods cause a rapid surge in blood glucose levels, which may then cause a quick release of insulin to counteract that rise. Low glycemic foods are optimal for supplying long-term sustained energy for children and adults without causing pendulous swings in blood sugar . Examples of low glycemic index foods include whole grain products, low-fat yogurt or milk, apples, and almost all vegetables and beans . The pre-event meal should be high in carbohydrate and low in fat so that it may be easily digested. Excess fat should not be consumed because it delays stomach emptying and takes longer to digest. Excess protein also should be avoided to prevent added stress on the kidneys. The meal should be eaten 3.5 to 4 hours before an event and provide 100 to 200 g carbohydrate for children and adolescents . Appropriate pregame meals include toast with jelly, a baked potato, spaghetti with tomato sauce, cereal with skim milk, or low-fat yogurt with fruit . Anyone who competes in all-day events should consume 1 g of carbohydrate/kg body weight for every hour of activity. Good sources include fresh fruits, energy bars, and sports drinks .
The 2 hours after competition represent the most critical time to restore muscle glycogen; synthesis is reduced by 66% when postexercise carbohydrate ingestion is delayed more than 2 hours . Athletes should consume at least 1.5 g of carbohydrate/kg body weight immediately after exercise and again 2 hours after exercise to maximize glycogen regeneration. Carbohydrates with a medium to high glycemic index should take priority in postexercise recovery diets. Good sources of these foods include white bread, raisins, bananas, sugar, carrots, pasta, honey, and sports drinks . A study by Burke and colleagues demonstrated that consuming high glycemic carbohydrate foods produced greater glycogen storage in the first 24 hours after exercise than did low glycemic index foods . Increased protein intake is also recommended for muscle repair and to further increase the glycogen resynthesis rate. Good foods to consume that have both protein and carbohydrates include peanut butter or cheese with crackers, trail mix, sports bars, and yogurt and granola. Guidelines recommend a 1:3 ratio of protein to carbohydrate consumption .
Elite athletes, recreational athletes, and sedentary people all require the same nutrients, although the amount of nutrients needed is influenced by age, sex, body size, activity level, and state of health . It is important for all athletes to consume a balanced diet that consists of approximately 50% to 65% carbohydrates, 20% to 30% fats, and 12% to 15% proteins to ensure health and performance. Proper nutrition in young athletes is vital to prevent inadequate energy intake, which may inhibit normal growth and development and overall performance.
The role of carbohydrates, proteins, and fats in athletic performance
Basic nutrition is vital for aiding in growth, providing energy, and achieving good health and school performance. Sports nutrition expands on these basic principles to enhance athletic performance by reducing fatigue and susceptibility to disease and injury while concurrently allowing an athlete to train harder and longer and recover faster . The underlying macronutrients that fuel physical activity are carbohydrates, proteins, and fats. It is crucial for athletes to take in equal or more calories than they are expending to prevent an energy deficit, which can result in loss of muscle mass, menstrual dysfunction, loss of or failure to gain bone density, and increased risk for fatigue, injury, or illness .
In order for any muscle to do work, adenosine triphosphate (ATP) is required; it also must be replenished continuously during physical activity in order for the activity to continue . When energy demands increase during exercise, the body relies on three different systems to transfer stored energy to ATP: the phosphagen, glycolytic, and aerobic systems . The phosphagen system uses stored phosphocreatine in muscle cells to directly produce ATP and is used primarily for short-term, high-intensity exercise, such as sprinting, high jumping, or a rapid weight lift. Myocytes can only store small amounts of phosphocreatine, however, and ATP production is limited accordingly. This system can only deliver enough ATP to support activity that lasts less than 20 seconds. The glycolytic system is also a short-term fuel provider and supplies ATP for intense activity that lasts from 20 to 45 seconds . Both of these systems are anaerobic, whereas the third system, oxidative phosphorylation, requires oxygen to produce ATP through the oxidation of carbohydrates, fats, and proteins. This system is used for activity lasting longer than 45 seconds .
In 2005, the government introduced a revision of their food guidance system. Originally, it was developed in 1992 as the food pyramid guide (FPG). “MyPyramid,” released in 2005, symbolizes a personalized approach to healthy eating and physical activity ( Figs. 1 and 2 ). It is recommended for everyone to obtain at least the lower end of the recommended range of servings, whereas the higher end is suggested for athletes who expend a significant amount of energy in physical activity. The Institutes of Medicine Food and Nutrition Board recently revised caloric recommendations as follows :
Male athletes aged 30 years and older
Total energy expenditure = 662 − 9.53 × age (years) + 1.48 [physical activity] × (15.91 × weight [kg] + 539.6 × height [m])
Female athletes aged 30 years and older
Total energy expenditure = 354 − 6.91 × age (years) + 1.45 [physical activity] × (9.36 × weight [kg] + 726 × height [m])
For male and female athletes between 19 and 30 years
Add 7 kcal/d for women and 10 kcal/d for men for every year before 30
For children and teens younger than 19 years
Boys/girls aged 7 to 10: 2000 calories/d
High school boys: 3000 to 6000 calories/d
High school girls: 2200 to 4000 calories/d
Carbohydrates are the primary source of fuel during exercise and contain approximately 4 kcal/g. An adult athlete’s diet should typically be made up of 60% to 65% carbohydrates, whereas an adolescent athlete’s diet should contain 55% to 60% . In 2002, the Institute of Medicine established the RDA of carbohydrates for adults and children as 130 g/d, which is based on the amount needed to supply the brain with adequate glucose . Beyond this specific RDA, they also set for carbohydrates an acceptable macronutrient distribution range of 45% to 65% of total caloric intake. Both of these guidelines are intended to meet the needs of 95% of the general population .
Carbohydrates taken in through food are necessary to maintain blood glucose and is stored as glycogen in the muscles and liver . Muscle glycogen is the fastest form of energy available to the working muscle and can be released up to three times quicker than energy from any other source . Muscle glycogen and blood glucose are also the limiting factors in any type of human performance . As exercise intensity increases, the more muscle glycogen is relied on as an energy source ; however, as the duration of exercise increases, the source of energy shifts from muscle glycogen to circulating blood glucose . During long periods of exercise, muscle glycogen and blood glucose levels both become low, and unless carbohydrates are replenished, an athlete will not be able to perform at a high level . A study by Ahlborg and colleagues found that work time to exhaustion was directly related to the quantity of initial glycogen stores in the working muscles. They showed that by manipulating the quantity of carbohydrate in the diet, the concentration of glycogen in the muscle could be altered, as could the athlete’s time to exhaustion.
Endurance athletes who train aerobically for more than 90 minutes daily need approximately 6 to 10 g of carbohydrate/kg of body weight/day to restore glycogen levels during training. This amounts to roughly 300 to 700 g of carbohydrate . Carbohydrate ingestion during exercise that lasts longer than 1 hour also may help increase endurance . Athletes can help maintain their body’s supply of energy by consuming approximately 25 to 30 g of carbohydrate every half hour during exercise. This practice can improve performance by maintaining blood glucose levels after muscle glycogen has been diminished, because 1 g carbohydrate/min is delivered to the tissues as fatigue sets in .
Proteins carry out many bodily functions and aid in the structure of skin, hair, nails, and muscle. Protein normally provides less than 5% of the energy expended at rest and during mild exercise . However, as exercise duration increases, proteins contribute to the maintenance of blood glucose via gluconeogenesis in the liver . Proteins contain approximately 4 kcal/g, similar to carbohydrates, and the current RDA for protein is 0.8 g/kg body weight/day for the general population.
Athletes may require a higher protein intake in the early stages of resistance and endurance training because of increasing muscle mass . In the beginning of training, the recommended protein intake is 1.5 to 1.7 g/kg body weight/day. As training enters the maintenance phase, protein intake may be decreased to 1.0 to 1.4 g/kg body weight/day. Protein requirements are necessarily greater in adolescents than in sedentary adults because of growth and development of lean body mass. The RDA of protein for active children and adolescents is 2 g/kg/d . Overall, the protein recommendation for active adults and children is 12% to15% of energy intake . Resistance training may require a higher protein intake, and weight lifters consume anywhere from 1.2 to 3.4 g/kg body weight/day . Bodily protein synthesis seems to be at a maximum in strength-training athletes who consume 1.4 g protein/kg body weight/day .
Consuming more protein than the body can use is unnecessary and should be avoided. This is an important guideline to remember as ergogenic aids and other supplements become increasingly popular in modern society. When athletes consume diets that are high in protein, they compromise their carbohydrate status, which may affect their ability to train and compete at peak levels. Taking large amounts of protein or amino acid supplements can also lead to dehydration, urinary loss of calcium, weight gain, and stress on the kidneys and liver because protein requires almost seven times more water for metabolism than fat or carbohydrates .
Fats are used as a secondary fuel source after carbohydrates. Fats provide necessary vitamins, are essential for menstrual function, and protect the internal organs. They contain 9 kcal/g and should make up 20% to 25% of an athlete’s diet. There is no specific RDA for fat intake, but it is recommended that athletes consume no more than is recommended for a sedentary person. Children and adults should take in no more than 10% saturated, 10% polyunsaturated, and 10% monounsaturated fats in their diet.
Fat is the major fuel for light- to moderate-intensity exercise (<60% VO 2max ). During low-intensity exercise that lasts longer than 30 minutes, there is a gradual shift away from carbohydrate metabolism with an increasing reliance on fat metabolism, or beta-oxidation, as the primary energy source . With training, the quantity of mitochondrial enzymes can increase, which in turn increases fatty acid oxidation. Glucose uptake, glycolysis, and glycogenolysis are then increasingly inhibited by free fatty acid oxidation within the skeletal muscle . Trained individuals are able to use fat stores more efficiently than untrained athletes, who rely more heavily on carbohydrate stores.
One aspect of performance unique to women and younger adolescents is their higher capacity for lipid oxidation . Women are believed to oxidize fat better than men because of fluctuating hormones in the menstrual cycle. These hormones dramatically influence substrate selection and most likely account for the reduced reliance on carbohydrates . Children and adolescents generally have higher levels of glycerol in their blood, which results in increased use of free fatty acids during exercise. Despite their increased lipid use, it is still recommended that an adolescent’s consumption of fats be no more than 30% of their daily caloric intake .
It is important for physically active children and adolescents to consume enough nutrients to meet their needs for growth, tissue maintenance, and physical and intellectual performance . It is difficult to establish specific recommended intakes, however, because of large individual variability. During growth spurts, adolescents should consume an additional 500 kcal/d above their usual intake . Carbohydrates do not seem to play as great a role for youth in exercise as for adults because of the submaximal glycolytic capacity characteristic of younger age . The RDA for carbohydrates in children and adolescents is at least 50% of total daily caloric intake. The children’s FPG (see Fig. 2 ) is a useful tool for ensuring adequate nutrition in the diet. It is important to remember that active children should consume the high end of the range of recommended servings for each food group.
Precompetition meals are essential for athletes to maintain energy levels for the exercising muscles during competition . In a study by Sherman and colleagues, cycling performance was improved by 15% when athletes consumed 4.5 g/kg body weight carbohydrate 4 hours before moderate-intensity exercise. Consuming 1 to 4.5 g of carbohydrate/kg body weight 1 to 4 hours before activity helps to maintain blood glucose levels during exercise and ensure adequate carbohydrate availability . It is not recommended for athletes to fast before competition because of the risk of their blood glucose levels decreasing during exercise and impairing performance .
A study by Thomas and colleagues also showed that the glycemic index of an individual’s food intake may affect performance. Cyclists who consumed low glycemic index carbohydrates (<60) 1 hour before pedaling to exhaustion had a significantly longer endurance time than individuals who consumed medium (60–80) and high glycemic foods (>80). High glycemic foods cause a rapid surge in blood glucose levels, which may then cause a quick release of insulin to counteract that rise. Low glycemic foods are optimal for supplying long-term sustained energy for children and adults without causing pendulous swings in blood sugar . Examples of low glycemic index foods include whole grain products, low-fat yogurt or milk, apples, and almost all vegetables and beans . The pre-event meal should be high in carbohydrate and low in fat so that it may be easily digested. Excess fat should not be consumed because it delays stomach emptying and takes longer to digest. Excess protein also should be avoided to prevent added stress on the kidneys. The meal should be eaten 3.5 to 4 hours before an event and provide 100 to 200 g carbohydrate for children and adolescents . Appropriate pregame meals include toast with jelly, a baked potato, spaghetti with tomato sauce, cereal with skim milk, or low-fat yogurt with fruit . Anyone who competes in all-day events should consume 1 g of carbohydrate/kg body weight for every hour of activity. Good sources include fresh fruits, energy bars, and sports drinks .
The 2 hours after competition represent the most critical time to restore muscle glycogen; synthesis is reduced by 66% when postexercise carbohydrate ingestion is delayed more than 2 hours . Athletes should consume at least 1.5 g of carbohydrate/kg body weight immediately after exercise and again 2 hours after exercise to maximize glycogen regeneration. Carbohydrates with a medium to high glycemic index should take priority in postexercise recovery diets. Good sources of these foods include white bread, raisins, bananas, sugar, carrots, pasta, honey, and sports drinks . A study by Burke and colleagues demonstrated that consuming high glycemic carbohydrate foods produced greater glycogen storage in the first 24 hours after exercise than did low glycemic index foods . Increased protein intake is also recommended for muscle repair and to further increase the glycogen resynthesis rate. Good foods to consume that have both protein and carbohydrates include peanut butter or cheese with crackers, trail mix, sports bars, and yogurt and granola. Guidelines recommend a 1:3 ratio of protein to carbohydrate consumption .
Elite athletes, recreational athletes, and sedentary people all require the same nutrients, although the amount of nutrients needed is influenced by age, sex, body size, activity level, and state of health . It is important for all athletes to consume a balanced diet that consists of approximately 50% to 65% carbohydrates, 20% to 30% fats, and 12% to 15% proteins to ensure health and performance. Proper nutrition in young athletes is vital to prevent inadequate energy intake, which may inhibit normal growth and development and overall performance.
Related posts:
 Strength Training Recommendations for the Young Athlete
Exercise for Preventing Childhood Obesity
Low Back Pain in the Adolescent Athlete
Shoulder and Elbow Injuries in the Adolescent Athlete
Acute Knee Injuries in Skeletally Immature Athletes
Psychologic Stress Related to Injury and Impact on Sport Performance
Strength Training Recommendations for the Young Athlete
Exercise for Preventing Childhood Obesity
Low Back Pain in the Adolescent Athlete
Shoulder and Elbow Injuries in the Adolescent Athlete
Acute Knee Injuries in Skeletally Immature Athletes
Psychologic Stress Related to Injury and Impact on Sport Performance
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


