CHAPTER 26 Nonunion of the Olecranon and Proximal Ulna
GENERAL CONSIDERATIONS
Nonunion of olecranon and proximal ulna fractures is a relatively uncommon complication with the use of current techniques of osteosynthesis.9,35,59 Although this problem is perhaps less common today than in the past, it continues to challenge the orthopedic surgeon. Olecranon and proximal ulna fracture nonunion can result in profound functional disability. Patients consistently report pain.55 Other features typically include some degree of instability or limitation of elbow joint motion.
The main predisposing factors for a nonunion of the proximal ulna are inadequate fixation, premature motion, smoking,7 or a combination of all of these.3,4,20,31,32,37,45,63,73,75
INCIDENCE
Nonunion of fractures of the proximal ulna and olecranon has been reported to occur in 5% of all olecranon fractures44 and about 5% of all nonunions.10,11,22 Within a 10-year period (1980 to 1990), 196 olecranon fractures were treated at the Mayo Clinic, and there were only two instances of olecranon nonunion (1%).55
Nonunion is also a recognized complication of the proximal osteotomy of the olecranon to expose a fracture of the distal humerus.70 From 1980 to 1990 at the Mayo Clinic, this complication occurred in only one such patient.55 Other authors have reported a high rate of olecranon nonunion in these patients. Gainor and coworkers30 studied 10 patients who had a transverse osteotomy of the olecranon for surgical exposure of a complex distal humerus fracture. Nine of the osteotomies were reconstructed with a large lag screw and tension band wire, and one with smooth pins and a tension band wire. Within an average follow-up period of 24 months, nonunion of the olecranon osteotomy occurred in three of the patients.30
DIAGNOSIS
A definitive clinical diagnosis of nonunion cannot be determined until a pseudoarthrosis is evident radiographically. Six months is usually the minimum accepted time before a definite diagnosis of nonunion may be considered. A slow union is an indolent union that maintains the radiographic appearance of the early stages of a healing fracture; the fracture line is visible, and no decalcification or sclerosis is present at the bone ends.44 Delayed union is described as fracture healing in which evidence of attempted union is present radiographically. Reactive hyperemia, early resorption of bone ends, and some widening of the fracture site are usually associated with delayed union.
Nonunion is assumed when all evidence of bone healing has ceased. The bone ends and medullary canals are capped, the endosteal blood supply does not extend across the fracture site, and sclerosis of the bone ends is present in at least 25% of patients.32,34 False motion and a varying radiographic defect between the bone ends also are usually present. If a visible fracture line is not present on the plain radiographs, a tomogram is helpful.
CLINICAL PRESENTATION
The term “nonunion,” although describing the pathologic condition, misrepresents the clinical problem. The integrity of the ulna plays an important role not only in the function of the joint but also in the articular surfaces and elbow stability. Clinically, tenderness is consistently reported. Some degree of instability and limitation of motion are the other clinical features of the olecranon nonunion.55 Yet it is important to note that a small percentage of patients may function well with the nonunited fracture.38
CAUSES
Ossification in the olecranon begins at two or more centers, and the growing epiphysis may be misinterpreted or confused radiographically with a fracture line or nonunion.62,66 Olecranon nonunion rarely occurs in children, but it may result when displaced fractures are unrecognized or when inadequate internal fixation results in loss of reduction.43,53
Bilateral congenital pseudoarthrosis of the olecranon has been reported with radiographic features distinct from the kind of congenital pseudoarthrosis of the forearm previously reported.16 A vascularized fibular graft has been reported as successful in this circumstance.2 Nonunion of the olecranon has been reported in an infant following a birth injury and in adolescent stress fractures.39,40,67,75,76 Fracture separation of a nonunited ossification center in three adults has been reported.38 Primary bone grafting is recommended in these cases because of the high incidence of fibrous nonunion following simple open reduction and internal fixation.38
Walker71 reported a case of painful unilateral physeal nonunion in an adult weight lifter. After failure of conservative treatment, surgical union was achieved, using tension band wiring augmented with autologous iliac crest bone graft. Unilateral olecranon physeal nonunion may have a mechanical etiology as opposed to a genetic etiology in individuals with bilateral physeal persistence.54 These types of fractures heal reliably with fixation.52
Generally children have a higher rate of periosteal response and union. Fracture healing in the older age group of patients is good despite the fact that their fractures tend to heal at a slower rate than those in the younger patient.11 Fracture healing may be slowed in the diabetic patient, in the patient undergoing irradiation treatment,21,33,60 in the adult with a stress fracture,51,52,54 or as a result of smoking.17
There are several predisposing factors to nonunion of olecranon fractures: (1) inadequate fixation or immobilization,23,74 (2) distraction, (3) compounding of fracture, (4) infection, (5) comminution,64,69 (6) loss of blood supply,14 (7) defects between the fragments or interposition of soft tissue, (8) abnormalities of the electro-chemical or cellular physiologic mechanisms involved in fracture healing resulting from smoking (Box 26-1),1,3,8,14,17,44,66 and (9) adverse events associated with total elbow replacement.42
BOX 26-1 Causes or Predisposing Factors Contributing to Nonunion of the Olecranon
Inadequate, nonrigid internal fixation
Defects between bone fragments
Following total elbow replacement42
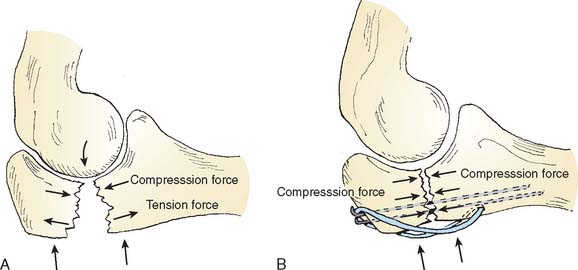
Technically, the most important factor in the treatment of either fresh fractures or nonunion of the olecranon is the need to convert the tensile forces arising from the forearm flexors and the triceps acting across the fracture or the nonunion site to a compressive force (Fig. 26-1).18,64 In tissue culture experiments, Bassett5,6 has shown that tension forces may prevent osseous precursors from forming cartilage or bone to promote the growth of fibrous tissue. Tension forces tend to produce an osteoclast-induced positive electrical potential that may interfere with bone healing. Compression forces, on the other hand, tend to effect an osteoblast-induced negative electrical potential that produces an enhancing effect on fracture healing.7,8,44
CLASSIFICATION
Generally, nonunions have been pathologically classified into two types, according to the biologic activity at the ends of the fracture fragments.36,50 The hypervascular type of nonunion has rich blood supply at the ends of the fragments and may be confirmed by increased technetium Tc-99m uptake. The avascular type has nonviable ends of the fracture fragments and also may be confirmed by a decreased technetium Tc-99m uptake.36,49,72
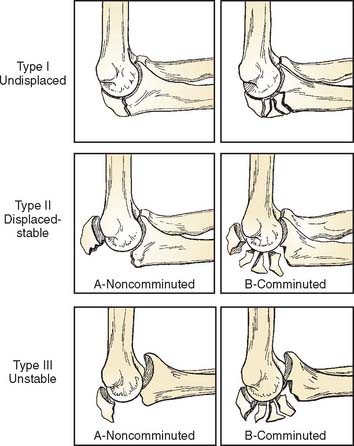
Nonunion of the proximal ulna distal to the insertion of the medial collateral ligament carries a better prognosis for reconstruction because the articular surface of the trochlear notch is intact.4,47,60 Any reconstruction for nonunion in an unstable injury at this level (Fig. 26-2) may need medial collateral ligament repair or reconstitution in addition to rigid internal fixation.47
TREATMENT OPTIONS FOR OLECRANON NONUNION
INDICATIONS
Asymptomatic nonunion with adequate elbow joint function requires no active treatment (Fig. 26-3). For symptomatic olecranon nonunion, the goals of treatment are the same as those of primary treatment for any displaced fracture: (1) to restore congruity of the sigmoid notch, (2) to restore or retain ligamentous stability, (3) to restore triceps extensor function, and (4) to restore mobility of the joint.

Nonunion of Monteggia fracture-dislocations requires special considerations.
Treatment of Infected Nonunion of the Olecranon
Muscle, myocutaneous, and vascularized fibular bone grafts have been used successfully in the treatment of nonunions.25 Successful use of a flexor carpi ulnaris local muscle flap has been reported by Meals46 and avoids the complications associated with microvascular repairs. The use of an external fixator or distraction arthroplasty is usually the most effective means of immobilization until soft tissue coverage and control of the infection can be achieved.
Treatment of Nonunion in Which Articular Cartilage Has Not Been Severely Damaged
Electrical Stimulation
If there is minimal displacement and if the overall alignment is acceptable, consideration might be given to electrical stimulation.7,8,13,56,61 A healing effect of electrical stimulation has been noted with coexisting low-grade infections. This noninvasive method can be used on an outpatient basis. However, the expense and the need to immobilize the joint have caused electrical stimulation to lose favor in recent years. The authors believe electrical stimulation is not a viable treatment option for olecranon or proximal ulna nonunions because of prolonged immobilization of the elbow joint, which is often already compromised by injury and which can lead to elbow stiffness.
Biologic Enhancement
The introduction of bone morphogenic protein (BMP-7) has been demonstrated to facilitate healing at several anatomic sites, including the olecranon region.26 Most heal within 4 to 5 months. This basic strategy is effective because the technology is becoming more refined, resulting in efficient delivery systems of effective product.
Excision
Encouraging early descriptions of the results of proximal fragment excision are available.22,27,29 In 1947, McKeever and Buck reported that 80% of the sigmoid notch could be excised without producing instability of the elbow joint (Fig. 26-4).45 Gartsman and colleagues31 found that restoration of elbow extensor function was equal after excision or fixation, as measured by static and dynamic strength testing. Excision of the proximal fragment with meticulous reattachment of the triceps tendon is an excellent option for treatment of an older patient with nonunion of a small avulsion fragment or a fragment involving less than 50% of the olecranon surface.31,37,45,47,73 Excision of nonunited fracture fragments is, of course, contraindicated in the growing child with an open proximal epiphysis.

TECHNICAL OPTIONS AND CONSIDERATIONS
Excision
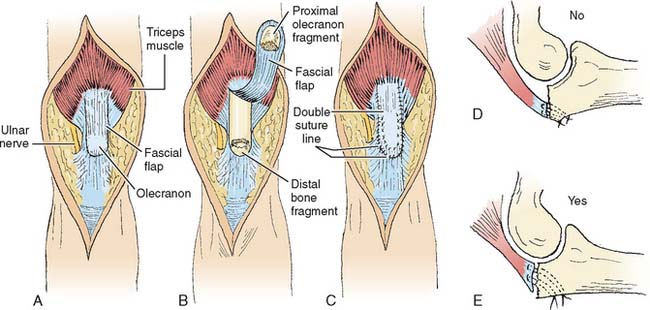
Small avulsion fragments are uncommon. Best results are obtained by simple excision and meticulous repair or advancement of the triceps tendon to the olecranon. Care must be taken to repair the medial and lateral retinacular portions of the triceps tendon using nonabsorbable suture material. Stay sutures should be placed directly through drill holes extending through the posterior cortex of the distal olecranon fragment (Fig. 26-5). The tendon margin is placed adjacent to the articular surface rather than to the posterior cortex. This improves the stability at the expense of a slightly decreased lever arm. Early active motion is permitted and encouraged 5 days after surgery through a range of 0 to 90 degrees, but flexion beyond 90 degrees should not be permitted for 4 to 6 weeks, depending on the extent of tendon advancement.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


