Fig. 16.1
Multiple rheumatoid nodules in a patient with advanced rheumatoid arthritis and destructive arthropathy of the hands

Fig. 16.2
Nodules and plaques of palisaded neutrophilic and granulomatous dermatitis in a somewhat linear configuration on the extensor forearm of a patient with rheumatoid arthritis
Differential Diagnosis
The differential diagnosis for rheumatoid nodules (RN) is broad [4, 5]. Acute rheumatic fever (ARF) is accompanied by subcutaneous nodules in 1 % of cases. ARF is associated with group A streptococcal pharyngitis. The location of the nodules over the olecranon and other joints is similar to rheumatoid nodules. Distinguishing features include that ARF nodules occur early in disease (first 1–3 weeks), tend to be smaller in size, and resolve spontaneously. There are individuals who develop rheumatoid nodules in the absence of rheumatoid arthritis (RA); these are referred to as “benign nodules.” Typically these occur in children on the scalp or posterior neck. Subcutaneous granuloma annulare is another entity that tends to occur in children or young adults and can present as subcutaneous nodules over joints. These have been referred as “pseudorheumatoid nodules.” Calcinosis cutis forms whitish, rock hard subcutaneous nodules over joints and is more common in scleroderma and dermatomyositis than RA. The Gottron’s papules of dermatomyositis occur over joints, but are violaceous and smaller than rheumatoid nodules. Tophi can mimic RN, but obviously occur in the setting of gout. Characteristic X-ray changes can be helpful to sort out the latter two entities. Multicentric reticulohistiocytosis occurs in middle-aged women, affects the skin and mucous membranes, and is associated with an erosive polyarthritis and increased risk of internal malignancy. There are multiple yellow-red papules that have a characteristic histology. A variety of xanthomas can occur as nodules over joints. They have a yellow-orange hue and are associated with abnormal lipids. Rheumatoid papules are distinctive because of their reddish-brown color, scale, and occurrence on the lower extremities. Approximately 10 % of SLE patients will have classic rheumatoid nodules that are clinically and histologically indistinguishable from nodules in an RA patient. Panniculitis typically affects larger areas of fat, is more amorphous than discrete nodules, and does not occur over joints. Similarly, medium vessel vasculitis such as polyarteritis nodosa typically occurs away from joints and may ulcerate, which RN do not. Infections tend to be more rapidly growing, tender, and may be associated with overlying erythema and suppurative ulceration. Urticaria is transient, and urticarial vasculitis is entirely macular without papules or nodules, so are easily distinguishable from RN.
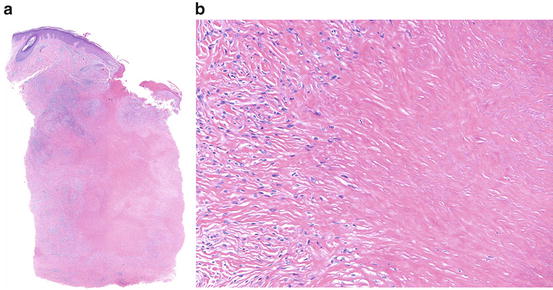
Histologic Features
Rheumatoid nodules when well developed display a palisaded granulomatous pattern involving the deep dermis and/or subcutis, with a nodular infiltrate of histiocytes surrounding a homogeneous and eosinophilic zone containing altered collagen and typically fibrin centrally [6–8] (Fig. 16.3). Vasculitis may be evident in early lesions and fibrosis in late lesions. Deep granuloma annulare may present a similar pattern, but generally contains mucin in the centers of palisaded foci.