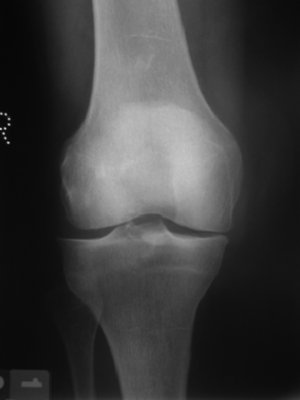
In addition to this, it often requires two radiographs in order to interpret meaningful information as an X-Ray is a two-dimensional image of a three-dimensional structure. Figures 11.2 and 11.3 show a loose body within the knee joint, which only becomes truly apparent in the lateral view (Figure 11.3).

Secondly, how useful is palpation in assessment and diagnosis? There is always a great temptation in assessing painful problems to go ahead and put a finger to the sore area and palpate. The problem here is that not all pain is felt at the site of origin; hence palpation can very often deceive. Soft tissues have the habit of referring pain to other areas; often they refer pain on a segmental basis. Referred pain is not too confusing if following the simple “rules” that appear towards the end of this chapter.
Following on from that, it should be obvious that any treatment needs to be directed at the source of, and not necessarily the site of, symptoms. There are, however, certain circumstances when the latter may be appropriate, but it cannot be assumed to be enough. For example, a client suffering with referred pain from tennis elbow (lateral epicondylitis) may require treatment to the source of problem, such as the bone-tendon junction, but may also benefit from pain relieving modalities such as TENS (transcutaneous electrical nerve stimulation). In this case, the treatment electrodes may be placed around the area of referred pain, not just the causal site. Treatment should have a beneficial effect on the particular tissues. Again this sounds obvious, but too often therapists have been guilty of performing treatments without really taking this into full consideration. The aims of treatment, therefore, should be to influence the cause of symptoms, not just relieve the symptoms.
Primary decisions for assessment
In the quest of diagnosis, there are some primary decisions to be made even before the assessment can begin:
- About which joint does the lesion lie?
- In what sort of tissue does the lesion lie? Contractile/inert
- Is the pain reproduced by the test?
The first question should really be answered by the initial subjective history. If the right sorts of questions are asked, then an initial impression may become evident, at least to the extent where the rehabilitator can decide at least which joint assessment to perform. The next two questions are answered by applying the Cyriax principle of selective tissue tensioning (Cyriax 1985a). Each tissue is selectively stressed, whilst at the same time not allowing any tension to occur at other tissues. Tissues are conveniently divided into two tissue types:
1. contractile: muscles, tendons and all corresponding junctions (musculo-tendinous and teno-osseous junctions)
2. inert: bones, cartilage, ligaments, capsule, bursae, fasciae, nerve root and dura mater.
One of the inert structures above also displays an additional characteristic that is significant in diagnosis, namely the joint’s fibrous capsule. Cyriax observed that joints lost their range of motion in predictable ways, which he termed Capsular Patterns:
When the capsule of a joint becomes inflamed, whether by trauma, infection or degeneration, it contracts and restricts the available range of movement in a set pattern. This pattern is the same for that joint but may be different for different joints, for example:
Shoulders display the same Capsular Pattern as each other, yet this differs from all knees.
A loss of range that is not in common with the known Capsular Pattern is called a Non-capsular Pattern.
Active, passive and resisted movements
Active movements are often not very helpful in diagnosis as all tissues are under tension simultaneously. However, they can give an indication of willingness to move, in addition to onset of pain, available range and end-feel to joint motion. Figure 11.4 shows active testing of shoulder flexion.

Passive movements stress the inert structures mainly, and provide an indication of onset of pain, range and end-feel. Passive movements should be exactly that; movements where the client is relaxed and does not attempt to help or join in with the movement. If this happens, then the client would be recruiting the contractile tissues, which may give a false positive result. Figure 11.5 shows passive testing of knee flexion.

Resisted movements put the contractile components under tension and give an idea of pain and strength. Resisted tests must be performed to the maximum, and should be isometric contractions in order to ensure that the inert structures are not stressed at the same time. In order to get maximum contraction, the joint needs to be in a relatively neutral position (to allow inert structures to be in a non-stretched position). This should be mid-range in order to allow the angle of force from the contractile unit to act in the most mechanically advantageous position, plus allows the optimum overlap between actin and myosin filaments for strong contraction. If only 90% strength is used, and the muscle lesion lies within the untested 10% of fibres, then a false negative result would be obtained by the test. Figure 11.6 shows resisted testing of the quadriceps.

Essentially, it should be remembered that all tests, whether passive or resisted, are only as sensitive and specific as the rehabilitator is at performing them; there is no substitute for practising assessment techniques.
Finally, it may be appropriate to use palpation in order to further localise the lesion. Further additional tests may then be carried out to aid this process in some cases; this simple form of assessment will allow the rehabilitator to gain a good clinical impression of diagnosis in 90% of cases. Figure 11.7 shows palpation of the peroneus brevis tendon.

End-feels
The normal feel to the end of passive joint range of motion is often called the end-feel. The following are classed as normal end-feels:
- Hard – usually due to bony opposition and feels like a solid immoveable block to movement (e.g. olecranon process meeting the olecranon fossa during full elbow extension).
- Soft – usually due to soft-tissue opposition, which feels like a squashing of a sponge (e.g. hamstrings meeting calf musculature during flexion of the knee).
- Elastic – usually the most common end-feel for synovial joints and is associated with stretching of the joint capsule and the feeling of elastic recoil when releasing the tension (e.g. lateral rotation of the shoulder joint).
Abnormal end-feels, or pathological end-feels as they indicate the presence of pathology, are as follows:
- Springy – usually due to the presence of cartilage being trapped between joint surfaces and feels like a firm resistance to movement that has some give when pressure is increased (e.g. meniscus in knee flexion or extension).
- Spasm – this is a hard end-feel caused by sudden activation of muscles in response to the movement through pain, or apprehension. It is different from a normal hard end-feel in that it is not always repeatable at the same point in the range of motion.
- Empty – this is when no end-range is actually reached either due to the onset of extreme pain, or because of major joint disruption (i.e. torn ligaments/capsule) which therefore offer no resistance to movement.
Referred pain
Referred pain is described as an error in perception; pain perceived elsewhere than at its true site is termed “referred”. The sensation of pain is an extremely complex phenomenon, and very subjective, however, certain aspects of pain perception are known (Butler 1991, 2000).
- site of pain – this is sensed by the body in the sensory cortex of the brain
- memory of pain – this is sensed in the temporal lobes of the brain
- degree of pain – this is sensed in the frontal lobes (amount of tension in these frontal lobes may govern the patient’s response to pain).
Referred pain, although complex in nature, can be said to follow some general rules (Cyriax 1985a):
- does not cross the mid-line of the body
- has a tendency to refer distally
- always refers segmentally (within a dermatome)
- may be felt in all or part of a dermatome
- is often felt or perceived as being deep.
The use of simple rules can help to make some sense of referred pain:
- usually, the deeper the site of lesion, the more vague the reference of pain and the greater the spread of reference
- this is also true of the location of the lesion; that is the more proximal, the more vague and increase in spread of reference
- in most cases, the stronger the stimulus, the increase in spread of reference.
Clinical orthopaedic examination
The following subheadings make the whole clinical assessment easier to breakdown for the purpose of greater understanding. Imagine the situation where an unknown client enters your clinic, requiring your professional services. After introducing yourself, you need to sit down with the client and glean a subjective history from them. The subjective history is literally exploring what the client feels has happened to themselves and how it is affecting them now. The objective examination, which comes after, allows the rehabilitator to perform a series of objective tests – namely passive and resisted movements. The process of assessment is attempting to put together several pieces of a puzzle, and to stand back and look at these and attempt to recognise the puzzle; it is rare that assessment yields every piece, so some sound anatomical knowledge and clinical reasoning skills will be needed for more complex patterns of clinical findings, and it is this particular skill that is hardest to gain. The rehabilitator looks for specific key elements (e.g. onset, behaviour and symptoms, etc.) in much the same way that a detective looks for key elements in any investigation (e.g. motive, opportunity, forensic evidence, etc.). Diagnosis is not, therefore, made on the basis of a single positive finding, but on a pattern of clinical features.
Subjective examination
The first stage of the subjective examination is that of observation.
Observation
- Face, posture and gait
It is particularly important to gauge how much pain and discomfort is the client in; one of the most accurate ways of doing this is to observe their face when they walk in the clinic, and when you greet them and introduce yourself to them. At this point, they are unaware that you may be observing them, and will tend to act in a more natural manner. The face can give clear indications of pain, whether severe, or prolonged, and may also give an idea of whether they have had disturbed sleep. It is a good opportunity to observe their posture also, and the way they move and walk. Someone with an ankle problem may walk on their heel with a relatively fixed and extended knee, whilst someone with a knee problem may well walk on their toes in order to prevent full knee extension.
The next stage is the interview stage.
Subjective history
During the subjective history taking, several questions need to be asked in order to help with the diagnostic process. The order of questions is ultimately a personal thing and does not have to follow the format set out below. It is worth noting, however, that it is highly likely that as a rehabilitator you are likely to not only ask someone to get relatively undressed, but you are going to invade their “personal space” by actually physically handling their limbs or body in some manner. In which case, it seems to me to be really important to gain some rapport with the client as quickly as possible, and hence ask questions about themselves of a more general (but no less important) nature early, and follow up with the most personal questions towards the end of the subjective interview. It may also be helpful as an aide memoir to use the keywords listed below as a template around which to ask relevant questions. These are linked together as pairs:
- age and occupation
- site and spread
- onset and duration
- behaviour and symptoms
- previous medical history and medication.
Age
Essentially, one of the first things required to establish is rapport, so to do that, you need to ask someone’s age. One of the useful things here is that some musculoskeletal conditions are age related, for example, slipped epiphysis in young adolescent boys, or degenerative conditions in the over 50s.
Occupation
Paired with age is occupation; it is important to establish exactly what the client does for a living. Are they a professional athlete of some kind, or are they a recreational athlete? Either way, you need to establish the activity levels they need to regain as part of your treatment plan. A professional athlete is likely to require more rehabilitation than an office worker who plays a little tennis at weekends. Equally, it needs to be established whether work or recreational activity may have any impact on the current injury – either causative or preventing recovery in some way.
Site
Asking the client to indicate where they feel their problem is can be enlightening in that it may indicate whether the problem is a local one, or indeed referred from elsewhere in the body. If one understands the rules of referred pain, then it can be seen that a client indicating medial knee pain with a vague wave of the hand around the area, is suffering from a different complaint to another client who indicated their medial knee pain with the pointing of one finger. In the latter case, it is likely that local pathology is allowing the client to localise the sensation somewhat more accurately than in the former case, where pain is referred to the knee from some pathology of the hip joint.
Spread
Linked to site of pain or symptoms, is that of spread. Ask the client: does their pain stay localised to the same area, or does it move in anyway? Again, knowledge of referred pain may further add to the evidence that the symptoms being experienced are from a referred source more proximal to the site of perceived pain.
Onset
It is always useful to attempt to find out what factors may have led to the onset of the client’s problem. Generally there are three forms of onset: gradual, sudden and insidious. The latter is a term that refers to an onset of unknown origin and can apply itself across both of the former two onsets (i.e. insidious gradual, or insidious sudden). Sudden onsets are usually associated with trauma, and as such a “mechanism of injury” may be established. Using sound anatomical and biomechanical knowledge, it may help to identify the tissues likely to be at fault causing symptoms. Gradual onsets may be the result of overuse, or repeated trauma (e.g. tendonitis). Examples of insidious insets may be pathologically more severe or even sinister; insidious gradual may be the onset of a tumour, insidious sudden may reflect a systemic problem such as gout.
Duration
This is an interesting one in that really it provides an idea of how likely you are to be able to change the client’s symptoms. Generally speaking, the longer someone has a condition, the less likely you are to be able to change or cure it. That does not mean to say that one should not attempt to change it; you may be the first therapist to be approached about the condition, or the first to accurately diagnose the problem.
Behaviour
What you are looking for here is: how do the symptoms change during the day, are they constant, and what aggravates and indeed what eases them? Is there any diurnal variation? That is, what are the symptoms like first thing in the morning, later in the day, at night? Conditions affecting the capsule and ligaments tend not to like extensive static periods and feel “stiff” when first moving, though feel better once moved. Tendonitis tends to be worse either during or after activity, whereas muscle lesions hurt on movements that recruit that particular muscle. It is rare for symptoms such as pain from musculoskeletal origin to be constantly present (this is often the manifestation of internal organ problems or systemic disease). Often, musculoskeletal pain is intermittent and movement dependant, and identifying what movements cause the onset of symptoms, and what positions, etc. cause relief, can help identify the tissue at fault. It may also help with provision of treatment in that someone who identifies that movement and application of warmth helps their knee, it would seem unwise not to incorporate some kind of heat treatment and mobilisation or exercise into their treatment/rehabilitation programme.
Symptoms
The most obvious symptom here is pain; however, some clients complain of other sensations, such as locking, giving way, pins and needles (paraesthesia) and even numbness (anaesthesia). They may also complain of stiffness (as a symptom, as opposed to lack of range of motion – which you would measure as objective sign). There are many authors who have written about pain and the types of pain that people experience, and relate this to the various types of tissue that give pain (Butler, 1991, 2000; Travell and Simons 1992; Simons et al. 1999). The fact that the pathophysiological mechanisms behind pain and its perception is so complex is further complicated when psychological influences are included (Butler 2000). This makes clinical reasoning of pain to become rather subjective and may lead to many opportunities for misunderstanding. For example, clients have described the pain of sciatica as “being like a red-hot poker down the back of my leg”, or sharp knee pain, “feeling like I have been stabbed”. As both the client and the rehabilitator need to fully understand what is meant by such descriptions, and either or both may misinterpret what is really being experienced, diagnosis based on such reasoning may be flawed. It would seem to suffice, therefore, when a client claims they have pain; objective and subjective examination will indicate the rest!
Previous medical history
Many therapists like to ask questions around this subject earlier in the interview; however this may result in digging up matter that is really quite personal, so leaving it to the end allows you first to establish rapport with your client. Again, there are many things to consider here; ideally keep it reasonably simple. Several forms of treatment are contraindicated by the presence of certain conditions, and there are too many to consider at this stage of assessment (as you have no idea what treatments you wish to perform at this stage). Therefore, ask the client whether they have had any previous major operations, accidents or illnesses. The common response to this is a glib, “No”. It is useful to check and ask, “Are you sure?” This has the purpose of just getting the client to realise that this is an important question that requires careful consideration. This may well yield the same response; however, you are more likely to be able to trust this response in terms of accuracy. A good example of the reason for asking such questions is this: a female client complains of low back pain of insidious gradual nature, and in her past history reveals she has had a hysterectomy. What needs to be established is why did she have a hysterectomy (was it due to cervical cancer – which can lead to spinal secondary metastases)? This can be ascertained by asking whether the client is still under the medical team for this, or has she been discharged (i.e. clear of the condition). This may help to change the potential worrying diagnoses of spinal cancer to one of remote possibility (note it does not dismiss the possibility).
Medication
Linked closely to past medical history is the question of medication. It may be useful to see if the client is taking any medication for the current condition, and whether or not it is beneficial. However, it is also another way of establishing whether there are any other underlying illnesses or diseases not disclosed in the previous questions. As there are a plethora of possible medications that clients use, we are particularly on the lookout for anticoagulants and long-term corticosteroid use. This is because in the case of the latter, ligaments and joints may become damaged by such medication; in the case of the former medication, potentially violent or high-impact treatment/rehabilitation processes may potentially cause bleeding that is not easy to stop (Grieve 1991).
Objective examination
The next stage is the beginning of the objective examination and should begin with a general inspection of the affected area.
Inspection
This is an opportunity to inspect the site of lesion briefly looking for evidence of the following:
- bony deformity
- colour changes
- wasting
- swelling.
Bony deformity could indicate joint subluxation, dislocation, fracture or postural changes, whilst colour changes may indicate presence of bleeding or signs of inflammation. Musculature associated with the site of lesion may indicate the presence of long-standing problems, or even neurological problems. Swelling would indicate the presence of an inflammatory process. Figure 11.8 shows a discrepancy in the relative scapula position from left to right.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


