8 Modified V-Y Quadriceps Turndown
A standard midline incision is the workhorse for total knee arthroplasty (TKA). It is well described in other areas of this text, and it enables tension-free patella ever-sion in a majority of primary TKA procedures. Exposure can become even more difficult in a revision setting with other factors such as condition of the skin, soft tissue contractures, patella position, and limited knee range of motion influencing knee and patella exposure. Although not often utilized, the modified V-Y quadriceps turndown is a necessary tool to have available for these most difficult of cases.1—3 Adapted by Dr. John Insall,4 this exposure allows excellent exposure as well as the ability to lengthen or shorten the extensor mechanism.
Indications
For additional exposure of the knee or patella joint total knee arthroplasty, V-Y quadriceps turndown aids in exposure when tibial tubercle osteotomy is elected to be avoided. Osteoporotic bone or poor distal skin quality may be factors that would influence a surgeon’s decision to avoid a tubercle tibial osteotomy since a typical osteotomy may lengthen the skin’s exposure by up to 8 cm.
Contraindications
This procedure is recommended after the failure of other methods of exposure and is not a primary exposure choice. The V-Y quadriceps turndown should not be selected until the standard midline incision with arthrotomy as well as a quadriceps snip has been attempted.
Special Instruments
No special instruments are needed. Arthrotomy is repaired with a heavy nonabsorbable suture at the close of the case.
Anesthesia
General anesthesia, epidural, or single shot spinal anesthesia
Patient and Equipment Positions
- Supine position
- Full range of motion of involved limb
- Tourniquet high on the thigh to allow appropriate extension for exposure if needed.
Surgical Procedure
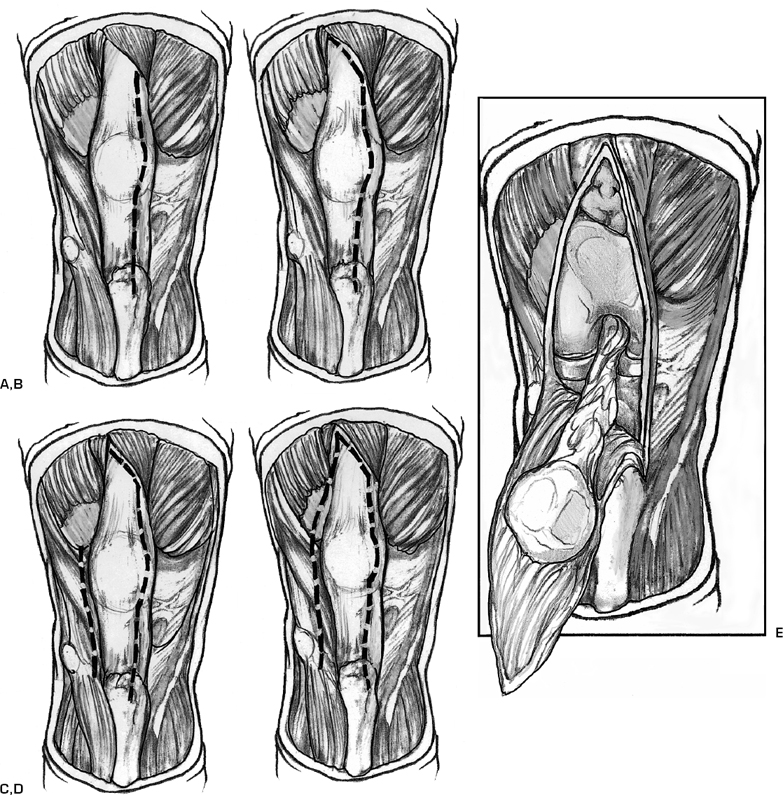
- Midline incision is performed crossing the medial border of the patella and extending distally 1 cm medial to the patella tendon insertion (Fig. 8–1A).
- Release of the lateral patella femoral ligaments is performed. This can be done easily at the insertion on the patella.
- Resection of the fat pad. Blunt dissection can aid in the detection of the patella tendon border.
- Patella exposure is evaluated. If excessive tension persists, a quadriceps snip can be performed. This is performed at an angle of 45 degrees in the lateral oblique direction and extended proximally (Fig. 8–1B).
- Check patella eversion. If still limited, hypertrophic scar or capsule can be excised.
- A lateral release can aid in the patella mobility. If still unsuccessful, the patella can be laterally displaced without eversion to achieve adequate exposure (Fig. 8–1C).
- If excessive tension persists, a modified V-Y turndown can be performed by connecting the lateral release incision at an angle of 45 degrees connecting the lateral release incision to the quadriceps incision (Fig. 8–1D,E).
A tendon is kept moist with a wet sponge throughout the procedure. The medial arthrotomy and quadriceps snip are repaired in a standard fashion using heavy nonabsorbable sutures. The lateral release portion can be left open to facilitate patella tracking.
Related posts:
 Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
 Total Knee Replacement: Medial Release via Osteotomy
Total Knee Replacement: Medial Release via Osteotomy
 Ligament Advancement in Total Knee Arthroplasty
Ligament Advancement in Total Knee Arthroplasty
 Ligament Injuries: Posterior Cruciate Ligament
Ligament Injuries: Posterior Cruciate Ligament
 Arthroscopic Abrasion Arthroplasty
Arthroscopic Abrasion Arthroplasty
 Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


