44
Metacarpal Head Fractures
Paul R. Greenlaw and Mark R. Belsky
History and Clinical Presentation
A 58-year-old right hand dominant woman presented for evaluation of an injury to the left hand. The patient had fallen on her left hand the previous day. Overnight she noted severe swelling in the left hand, which was treated with ice and ibuprofen. She complained of only left hand pain and denied paresthesias or paralysis in the left hand at presentation.
Physical Examination
The patient’s pertinent findings were confined to the left hand. Swelling and tenderness with intact skin were noted around the heads of the fourth and fifth metacarpals of the left hand. Range of motion of the fourth and fifth metacarpophalangeal (MP) joints was limited secondary to pain. Sensation and circulation were intact in the left ring and small finger with adequate alignment and rotation of the digits. No collateral ligament instability was appreciated.
Diagnostic Studies
Anteroposterior, lateral, and oblique radiographs of the left hand (Fig. 44–1) revealed a nondisplaced shear fracture of the fourth metacarpal head and a displaced sagittal fracture of the head of the fifth metacarpal extending into the metacarpal neck.
Differential Diagnosis
Fracture
Intraarticular
Extraarticular
Sprain
PEARLS
- The goal of ORIF is to obtain anatomic reduction of the joint surface with fixation that will allow early motion.
PITFALLS
- Small fragments require meticulous handling to avoid devascularization and resultant avascular necrosis.
Diagnosis
Sagittally Oriented Fifth Metacarpal Head Fracture with Extension into the Fifth Metacarpal Neck and Nondisplaced Shear Fracture of the Fourth Metacarpal Head
Metacarpal head fractures are uncommon fractures. A comprehensive review by McEl-fresh and Dobyns revealed an array of metacarpal head fracture patterns they classified into 10 types based on anatomic involvement as seen on roentgenographic examination: (1) epiphyseal, (2) collateral ligament avulsion injuries, (3) osteochondral, (4) oblique (sagittal), (5) vertical (coronal), (6) horizontal (transverse), (7) comminuted, (8) intraarticular extension (in boxers), (9) loss of substance, and (10) avascular necrosis. Of these types, comminuted fractures were the most common (31%).

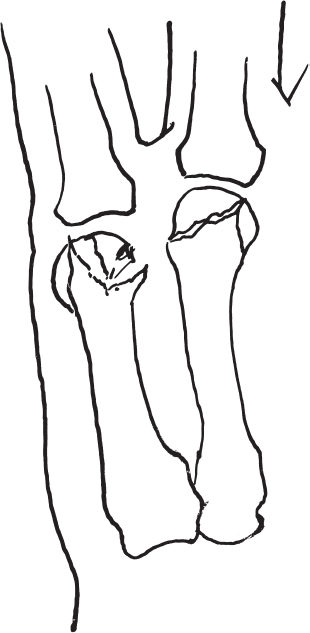
Figure 44–2. A stable fourth metacarpal head fracture and displaced fracture of the head of the fifth metacarpal.
Surgical Management
The patient was placed in an ulnar gutter splint and prepared for surgery. At surgery the following day an open reduction and internal fixation (ORIF) of the left fifth metacarpal head fracture was performed. Using fluoroscopy, the hand was examined, and revealed displacement of the radial sagittal portion of the head of the fifth metacarpal with comminution at the metacarpal neck. The fourth metacarpal head fracture appeared nondisplaced and stable.
Under axillary anesthesia and upper arm tourniquet, a curvilinear incision was made over the MP joint of the left fifth finger, the skin was incised, and the flaps reflected. The extensor tendon was mobilized by excising a portion of the sagittal band. The capsule was incised, and a hematoma was irrigated out of the joint. The comminuted fracture through the head of the fifth metacarpal with displacement of the radial portion of the radial side of the head was identified (Fig. 44–2).
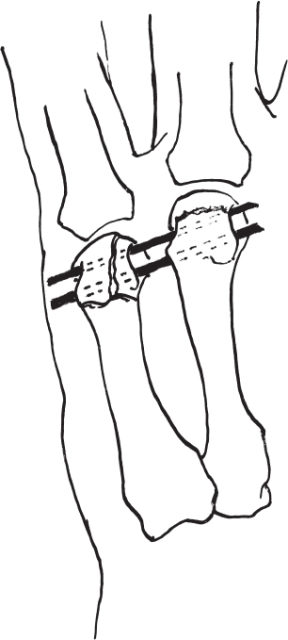
Under direct vision an open reduction was performed. The fracture fragment was held with two transverse 0.035-inch Kirschner wires (K wires) cut off subcutaneously (Fig. 44–3). An additional longitudinal 0.035-inch K wire was introduced through the head and down the shaft, reducing and maintaining the metacarpal head on the metacarpal shaft (Fig. 44–4). This wire was also cut off subcutaneously. The wound was irrigated, and then the capsule and skin were closed. The patient was placed in a solid short-arm cast extending to incorporate the ring and small fingers.