Fig. 18.1
Heart and thoracic aorta. Focal pigmentation on the mitral and aortic valve and sporadically in the subendocardial layer of the myocardium. Ulcerative arteriosclerosis and numerous pigmented foci, especially at the places of atherosclerotic plaques in the aorta

Fig. 18.2
Aortic cusp of the mitral valve. View from below. Pigmentation in insertion part and at the place of the origin of heart strings

Fig. 18.3
Semilunar valves of the aorta. Considerable pigmentation and calcification of insertion part became more pronounced after the removal of valves
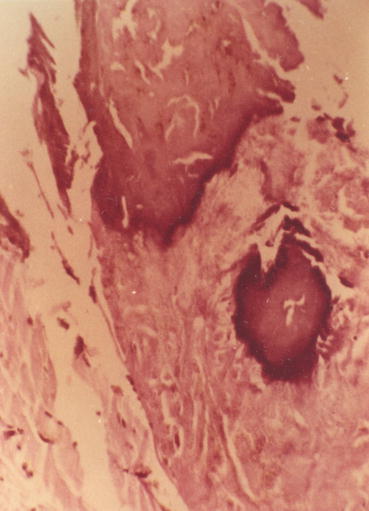
Fig. 18.4
Extensive calcification and pigmentation in basal part of the aortic valve (haematoxylin eosin staining, 260-fold magnification)
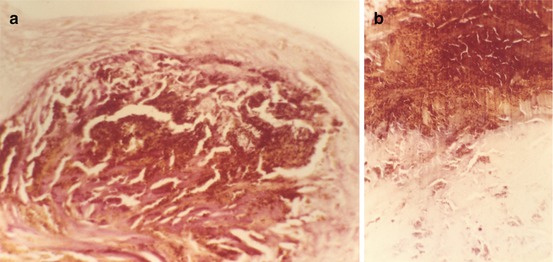
Fig. 18.5
(a, b) Massive pigmentation in the fibrous annulus of the aortic valve (haematoxylin eosin staining, 130-fold magnification)
Fig. 18.6
Large calcification in the pigmented area of the fibrous annulus of the aortic valve (haematoxylin eosin staining, 130-fold magnification)
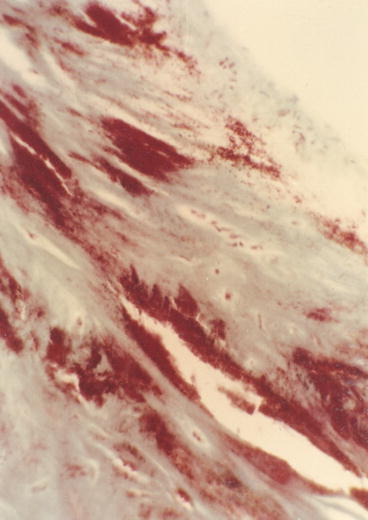
Fig. 18.7
Pigment masses in the fibrous annulus of the mitral valve (trichrome green staining, 130-fold magnification)
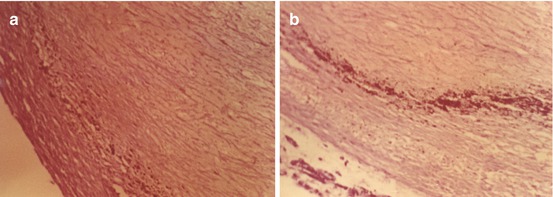
Fig. 18.8
(a) Pigment granules in the area of the lamina elastica interna of the coronary artery. (b) Marked pigment deposition in the area adjacent to atherosclerotic plaque (cresyl violet staining, 260-fold magnification)
Fig. 18.9
Sclerotic stenosis of the coronary arteriole with pigment deposits in the wall. Fibrosis and pigmentation of adjacent areas (haematoxylin eosin staining, 260-fold magnification)
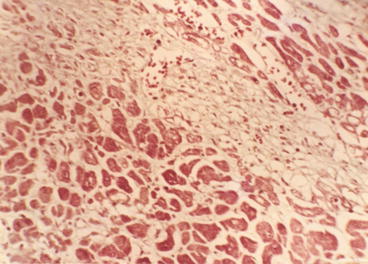
Fig. 18.10
Fragmentation, vacuolar degeneration and focal fibrosis in the myocardium (trichrome green staining, 160-fold magnification)
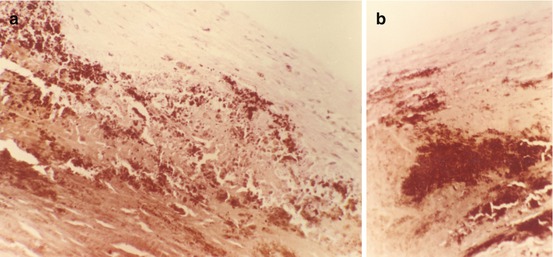
Fig. 18.11
(a, b) Massive pigmentation of the aortic media in the area of atherosclerotic plaque (haematoxylin eosin staining, 130-fold magnification)
Alkaptonuria frequently results in significant cardiovascular lesions, particularly aortic stenosis. There is also intensified arteriosclerosis, ochronotic nephrosis and the formation of urinary calculi as additional adverse effects of pigment deposition.
Ochronotic pigment deposition in cardiovascular system may be of clinical importance (Brueck et al. 2008). The pigment is distributed in the walls of blood vessels generally and particularly the aorta, arteries of both large and small dimension, arterioles and capillaries as well as in other, relatively collagenous or avascular connective tissues like the pericardium, valve cusps and rings and organising myocardial infarctions (Figs. 18.1, 18.2, 18.3, 18.4, 18.5a, b, 18.6, 18.7, 18.8a, b, 18.9, 18.10 and 18.11a, b). In the walls of the larger arteries, the pigment deposits can be associated with accentuated arteriosclerosis and in the heart valves with calcification, which may result in aortic stenosis (Concistre et al. 2011).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


