14. Lower respiratory tract infections



Epidemiology
The lower respiratory tract refers to the part from the trachea to the lungs and includes the larynx. The mucociliary escalator (see Ch. 13) ensures that the complex and abundant bacterial flora of the upper tract is much reduced in the larynx and trachea, and the bronchi in health are sterile.
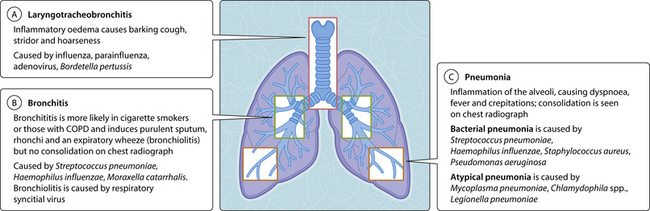
Respiratory tract infections are the most frequent cause of GP consultation, of which pneumonia only accounts for approximately 10% (Fig. 3.14.1). Patients with chronic obstructive pulmonary disease (COPD) are at risk of acute exacerbations of bacterial bronchitis when acquiring a viral infection. Respiratory syncytial virus causes bronchiolitis in infants who are less than 2 years of age and can cause life-threatening pneumonitis in the immunosuppressed host (e.g. transplant recipient). Influenza may be complicated by superinfection with bacteria, especially pneumococcal and staphylococcal pneumonia. Influenza vaccine should be given to all ‘at-risk’ persons in the autumn, and the drug oseltamavir is available. Pertussis tracheobronchitis (whooping cough) occurs in communities with low vaccination coverage, and spread may be reduced by early treatment with erythromycin. Bacterial (typical) pneumonia develops when bacteria overwhelm the bronchial host defences and is more common in the elderly. Mycoplasma, Chlamydophila spp. and Coxiella burnetii (causes of atypical pneumonia) can infect the previously healthy. Legionella pneumophila has its reservoir in warm water and is spread by aerosol, such as those created by poorly maintained showers and air-conditioners. Typically it affects the borderline immunocompromised, for example heavy-drinking, heavy-smoking elderly persons returning from warm climates.
< div class='tao-gold-member'>
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


