Chapter 26 Lower limb orthoses
Lower limb orthoses, with their many variations, are among the most commonly prescribed biomechanical devices intended to assist individuals with neuromuscular deficits.15 The preponderance of lower limb devices in clinical use reflects both the strong desire by most individuals with a physical disability to achieve independent mobility in the community and the fact that present orthotic technology often does a reasonably effective job of restoring gross physical functions such as walking and standing. For athletes, subtle interventions with foot orthoses sometimes overcome small physiologic deficits that otherwise might impede performance. Therefore, lower limb orthoses are applicable to enhance function for many biomechanical deficits, both large and small.
Custom footwear and modifications to commercial footwear are extremely important aspects of orthotic and pedorthic practice. Not only can shoe adaptations successfully treat many simpler problems, but they also can significantly enhance the effectiveness of orthotic management when more proximal devices are required.9 The shoe and its functions are discussed in more detail in Chapter 24.
Foot orthoses
Conceptually FOs usually are divided into three broad categories33:
Intermediate FOs made of semirigid materials are popular clinically because they can be fabricated from multiple layers of materials of slightly different densities to provide graduated degrees of control, thereby enhancing client acceptance. OTC, prefabricated, or modular intermediate FOs may suffice for mild problems such as metatarsalgia without ulceration. These somewhat generic devices also may be suitable for a clinical trial to verify the effectiveness of orthotic management in a given case. Chronic conditions as well as moderate and severe problems, including all feet with a history of ulceration or sensory limitation, typically require custom-molded devices to ensure the most meticulous fit.
Corrective FOs made of rigid materials can be extremely difficult to fit successfully and require meticulous attention to detail.2 A weaning period of several weeks is commonly recommended for client acceptance. Most orthotists and pedorthists reserve the use of rigid materials for easily correctable, flexible deformities such as mild ankle valgus, and for subtle control of a nearly normal foot with slight biomechanical deficits, such as slight excess pronation in a distance runner.
Ankle–foot orthoses
Ankle–foot orthoses (AFOs) can be designed with sufficient mechanical lever arms to effectively control the ankle complex and to influence the knee joint indirectly, making them applicable for the management of more extensive disabilities than can be managed with FOs. Successful use of electronic AFOs based upon electrical stimulation of weak or paralyzed muscles has been reported with increasing frequency in recent decades.13 In the United States, commercial versions of orthoses that incorporate neuromuscular electrical stimulation (NMES) recently have become clinically available.31
When a mechanical AFO is desired, the clinician must choose from among metal alloy devices, plastic devices, and a hybrid assembly incorporating both materials. In most cases, such technical decisions are best left to the orthotist and patient, who can take the time to fully discuss the various advantages and disadvantages of each approach. In general, plastic or hybrid plastic/metal systems predominate in North America because of the greater degree of client acceptance and circumferential control they offer.18 Carbon fiber composite AFOs that are thinner, lighter, and stronger than thermoplastic devices are now available. Composite AFOs have been very well accepted by patients and offer improvements in range of ankle motion and push-off characteristics.7 Unfortunately, funding restrictions continue to prevent many good candidates from having access to the most modern orthotic technology and effectively discourage the development of more advanced future orthoses.
Minimal contact designs are sometimes best for persons with fluctuating edema and for heat-sensitive individuals who cannot tolerate the more intimately fitting plastic contours.23 Some clinicians prefer metal systems for growing children because of their adjustability for growth, but many others believe that plastic or hybrid devices are just as versatile in this regard.24 One of the most significant factors in material selection is client (or parent) preference, which largely determines acceptance and therefore should predominate over all moot points in the final decision.
Functionally, all orthotic devices including AFOs must achieve one or more fundamental goals, such as4 (1) control of motion, (2) correction of deformity, and (3) compensation for weakness. Figure 26-1 illustrates one common application of control of motion: a rigid, plastic AFO with the ankle locked in slight dorsiflexion and a well-padded anterior proximal segment to stabilize the tibia. This design, first reported in 1969 by the Israeli orthotist Saltiel, is often colloquially termed a floor reaction AFO28 because the extended, rigid forefoot section accentuates the knee extension moment at midstance and thereby prevents tibial collapse that otherwise would result from weak or absent gastrocnemius–soleus strength. This illustrates one of the critical treatment principles of orthotic management: The orthosis may indirectly affect remote body segments, and this characteristic can be used therapeutically. The sagittal plane biomechanics of this AFO at midstance are shown in Figure 26-2.

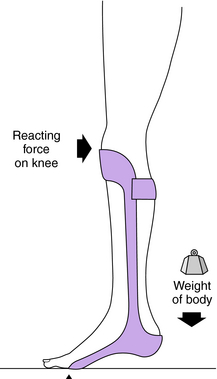
Orthoses can be rationally and succinctly prescribed based on the biomechanical function desired.19 The plastic floor reaction AFO with ankle locked in slight dorsiflexion usually is applicable when the patient has a paralyzed ankle–foot complex but good or better quadriceps and balance. Examples of pathologies that could result in this clinical picture include myelodysplasia, spinal cord injury, peripheral nerve injury, poliomyelitis, and gastrocnemius–soleus trauma or dysfunction.
One of the more common lower limb deficits is a flaccid equinus, which may result from many causes, including Charcot-Marie-Tooth disease, cerebrovascular accidents with mild residual symptoms, muscular dystrophy, and peroneal palsies of various types. The orthotic options to compensate for pretibial compartment weakness or paralysis definitively (Fig. 26-3) include the following:
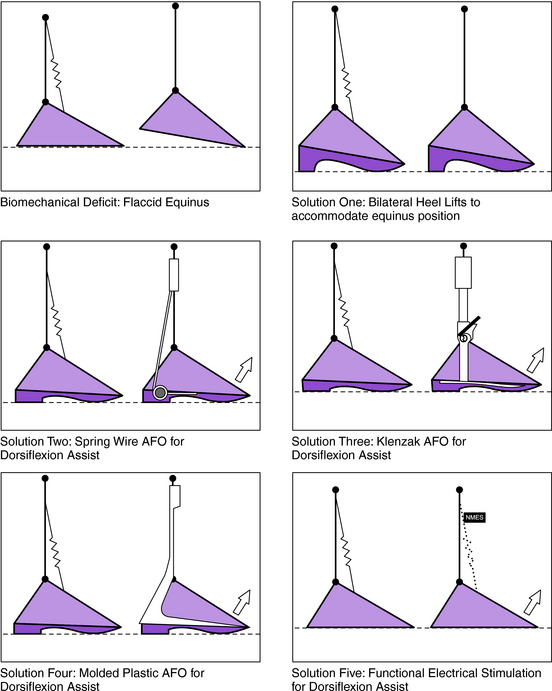
A functionally based prescription, such as “orthosis to compensate for weakened pretibial musculature,” ensures that the orthotist considers all available alternatives before determining the optimum solution for a particular patient.23 A more restrictive prescription, such as “prefabricated plastic AFO to provide dorsiflexion assist,” is appropriate only if that is the sole desirable solution—and all others are automatically ruled out.
The fifth option (NMES) recently has become commercially available in the United States. Although the biomechanical result (increased toe clearance during swing) is similar among all AFO designs, potential additional benefits from electronic AFOs30 include the following:
< div class='tao-gold-member'>
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


