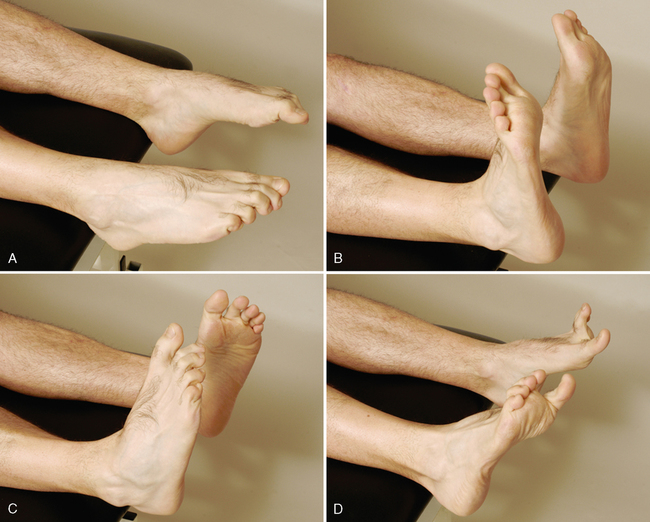
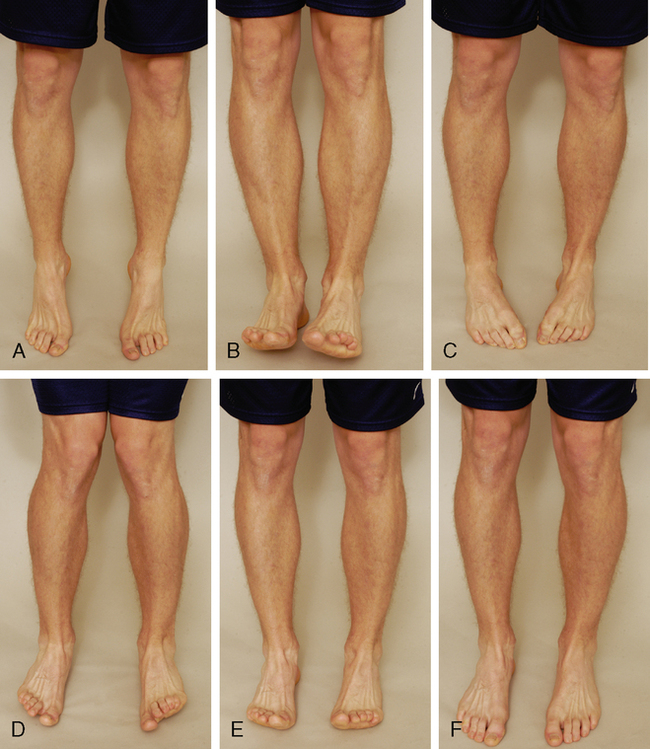
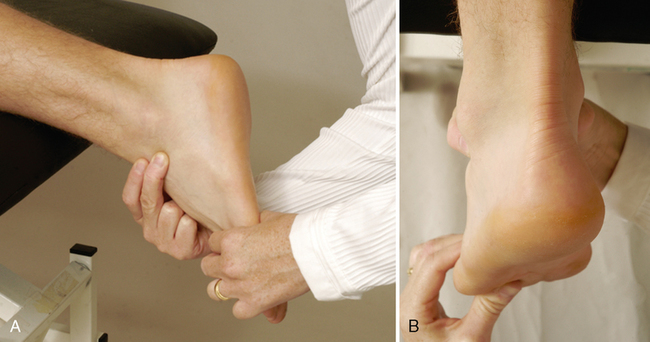
CHAPTER 12 Active movements of the lower leg, ankle, and foot should be done in both weight-bearing and non-weight-bearing positions (long leg sitting or supine lying), and the examiner should note any differences, because foot deformities and deviations, in addition to decreased range of motion (ROM), can lead to injury in other parts of the lower kinetic chain and spine.1 INDICATIONS OF A POSITIVE TEST Plantar flexion of the ankle is approximately 50°. If the ROM is less than this or is less than for the unaffected leg, the movement is restricted for some reason. The patient’s heel normally inverts when the movement is performed in weight bearing. If heel inversion does not occur, the foot is unstable, or tibialis posterior weakness or tightness is present.2–4 The tibialis posterior muscle and tendon balance the pull of the peroneal muscles, protect the spring ligament, and invert and stabilize the hindfoot during toe-off.5 • Talar position tests are not designed to identify specifically any particular pathological condition; rather, they identify anatomical and biomechanical abnormalities that contribute to a pathological condition. That pathology may occur locally at the foot and ankle or remotely at areas such as the back, knee, or hip. The overall prevalence of malalignment reported in the literature ranges from 10% in the Cheshire Foot Pain and Disability Survey in the United Kingdom to 28% in the Framingham Foot Study in the United States. Clinically, it has been hypothesized that abnormal talar alignment and mechanics can result in pathological conditions of the foot. Regardless of the prevalence of foot pain, the cause-and-effect relationship between talar position and pathological conditions has yet to be definitively determined.6–10 RELIABILITY/SPECIFICITY/SENSITIVITY COMPARISON11–16 NEUTRAL POSITION OF THE TALUS (PRONE)11–13,17–20 NEUTRAL POSITION OF THE TALUS (SUPINE)14,15,17–20 NEUTRAL POSITION OF THE TALUS (WEIGHT-BEARING POSITION)11,13,16,18,21,22 • Mueller et al.13 described a progression of neutral talus positions in standing (i.e., the navicular drop test) to quantify midfoot mobility and its effect on other parts of the kinetic chain. With a small, rigid ruler, the examiner first measures the height of the navicular from the floor in the neutral talus position, using the most prominent part of the navicular tuberosity; the height of the navicular in normal relaxed standing then is measured. The difference, called the navicular drop, indicates the amount of foot pronation or flattening of the medial longitudinal arch during standing. Any measurement greater than 10 mm is considered abnormal. Few population-based studies have examined the prevalence of foot pain in the general population. Causal relationships between specific malalignments and injuries have been difficult to verify. In a random sampling of people in Australia, foot pain affected nearly 1 in 5 individuals. The pain was associated with increased age, female gender, obesity, and pain in other body regions, and it had a significant detrimental impact on health-related quality of life. The overall prevalence reported in this study was higher than that reported in the Cheshire Foot Pain and Disability Survey in the United Kingdom (10%). However, it was lower than the prevalence rates reported in two studies in the United States: the National Health Interview Survey in the United States (24%) and the Framingham Foot Study (28%).6–10
LOWER LEG, ANKLE, AND FOOT
SELECTED MOVEMENTS
SPECIAL TESTS FOR NEUTRAL POSITION OF THE TALUS
Relevant Special Tests
Suspected Injury
Epidemiology and Demographics
Mechanism of Injury
Validity
Interrater Reliability
Intrarater Reliability
Neutral position of the talus (weight-bearing position)
Unknown
0.15-0.79
0.14-0.85
Neutral position of the talus (supine)
Unknown
Unknown
Unknown
Neutral position of the talus (prone)
Unknown
0.25
0.06-0.77




SPECIAL TESTS FOR ALIGNMENT
Relevant Special Tests
Epidemiology and Demographics
LOWER LEG, ANKLE, AND FOOT