CHAPTER 54 Linked Total Elbow Arthroplasty in Patients with Rheumatoid Arthritis
INTRODUCTION
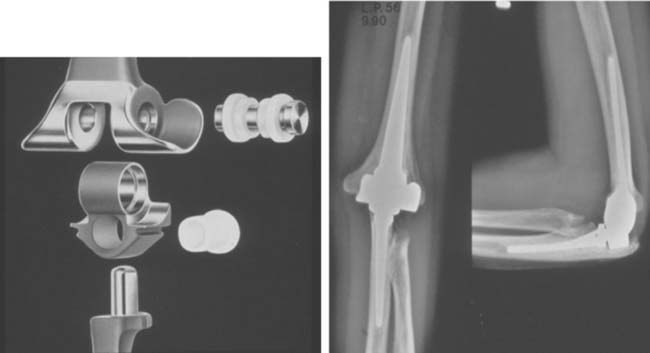
Both coupled and uncoupled elbow replacement prosthetic designs are employed for the management of end-stage rheumatoid arthritis.11,12,43 This chapter reviews the results of the linked, semiconstrained design, primarily that of the Coonrad/Morrey. As noted previously in this text, the clinical and radiologic presentation of inflammatory arthritis in general and rheumatoid arthritis in particular varies considerably (Fig. 54-1). The semiconstrained implant is especially useful in the type III and IV presentations because this design philosophy assesses stability in the face of bone loss and joint laxity2 (Fig 54-2).

FIGURE 54-1 The spectrum of radiographic presentation from grades I to V in patients with rheumatoid arthritis after Connor and Morrey9 and Morrey.33

To date, several evaluation systems exist that allow a critical assessment of the elbow when affected by disease and after therapeutic intervention (see Chapter 5). In the past, we employed the Mayo Elbow Performance Score (MEPS) as defined in Table 54-126 and are currently incorporating the measurements of the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire as well.
TABLE 54-1 Mayo Elbow Performance Score*
| Function | Point Score |
|---|---|
| Pain (45 points) | |
| None | 45 |
| Mild | 30 |
| Moderate | 15 |
| Severe | 0 |
| Motion (20 points) | |
| Arc 100 degrees | 20 |
| Arc 50 to 100 degrees | 15 |
| Arc 2 degrees | 5 |
| Stability (10 points)† | |
| Stable | 10 |
| Moderate instability | |
| Gross instability | 0 |
| Daily function (25 points) | |
| Combing hair | 5 |
| Feeding oneself | 5 |
| Hygiene | 5 |
| Putting on shirt | 5 |
| Putting on shoes | 5 |
| Maximum possible total | 100 |
* 90 points or more = excellent; 75 to 89 points = good; 60 to 74 points = fair; and less than 60 points = poor.
† Stable = no apparent varus-valgus laxity clinically; moderate instability = less than 10 degrees of varus-valgus laxity; gross instability = 10 degrees or more of varus-valgus laxity.
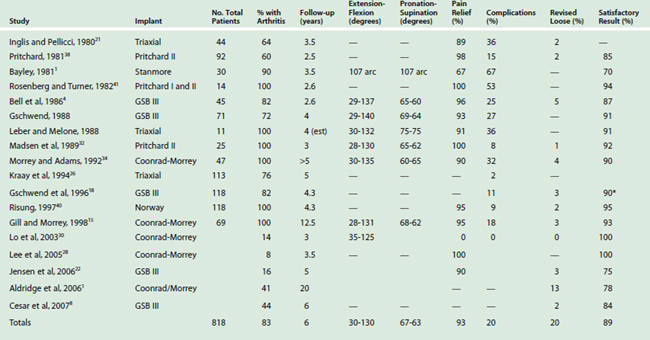
Review of the literature reveals improving and encouraging results with several semiconstrained designs (Table 54-2).16 In this chapter, we review several of these experiences and then focus on Mayo’s perspective and outcomes. The outcome of replacement for rheumatoid is superior to that for traumatic arthritis.3
HISTORICAL PERSPECTIVE
THE PRITCHARD PROSTHESIS
The Pritchard II prosthesis (Fig. 54-3) was an early design introduced in the 1970s as a linked semiconstrained device.32,38,39 Pritchard’s own experience with 92 patients was reported in 1981 and included 55 with rheumatoid arthritis. The mean follow-up was short (2.5 years). Although the range of motion, stability, and measure of function were not reported, relief of pain was reported as 98%.38 A 15% complication rate and 2% loosening requiring revision were recorded.

Subsequently, Madsen and associates32 followed 25 consecutive Pritchard II implants for a mean of 3 years. Twenty-three of 25 patients had relief of pain. The flexion arc averaged 28 to 130 degrees and pronation-supination was 65 to 62 degrees, respectively. Stability was not discussed, but the mean assessment score improved from 40 to 82. However, radiographic loosening occurred in 6 of 24 elbows, and two necessitated revision.
These initial reports of the Pritchard II implant were of small numbers, and their findings were regarded as preliminary.32,38,39 The major problem was wear or fracture of the polyethylene bearing. The device was subsequently modified but is not used to any extent today.
THE TRIAXIAL DEVICE
There has been a tendency for wear and dislocation over time; however,13 this articulation has undergone numerous modifications but still allows several degrees of varus-valgus and axial rotation “play” (Fig. 54-4). The implant has been used almost exclusively for patients with rheumatoid arthritis. A customized version has been described for various pathologic states other than rheumatoid arthritis.

RESULTS
In the past, several reports emanating from the designing institution have documented the use of several variations of this design for rheumatoid arthritis. In general, a 90% satisfactory result is reported with follow-up less than 5 years.21 In one large series, Kraay and associates26 reviewed the outcome of 113 patients. Of these, 86 had rheumatoid arthritis. With surveillance averaging 5 years, five devices had failed owing to sepsis, but only two had been revised because of aseptic loosening. The 3- and 5-year survival rates were 92% and 90%, respectively, but the outcome has subsequently deteriorated owing to instability occurring when the bushing wore.
GSB III PROSTHESIS
The current GSB II device provides about 4 degrees of varus-valgus toggle and uniquely some axial translation (Fig. 54-5). The stem is stabilized by medial and lateral flanges that are attached to the condyles. Hence, a requirement of this implant is intact or reconstructed condyles. Experience with the modified implant was reported by Bell and colleagues4 in 1986. Forty-one of 46 patients had relief of pain, and range of motion averaged 29 to 137 degrees. In 1988, Gschwend and associates17 updated this experience, with the majority of patients having rheumatoid arthritis. Fifty-three of 57 patients had relief of pain; extension-flexion improved from 29 to 140 degrees, with pronation-supination increasing 68 to 64 degrees, respectively. In five elbows, there was a nonprogressive radiolucency. Overall, 27% of the elbows had complications, including four requiring excision arthroplasty. Seven elbows disarticulated during follow-up.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


