CHAPTER 53 Linked Elbow Arthroplasty: Rationale, Indications, and Surgical Technique
INTRODUCTION
As noted in Chapter 52 and further described in Chapters 54 through 60, the results of total elbow arthroplasty are improving with increased basic knowledge of elbow mechanics,24 better designs, and greater surgical experience.21 The general principles of the surgical technique and improved designs2,9,14,18,24 and a detailed description of my specific method of inserting the Coonrad-Morrey implant are presented. The results of semiconstrained joint replacement arthroplasty emphasize the Mayo Clinic experience with the modified Coonrad device.
RATIONALE
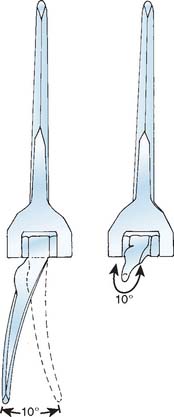
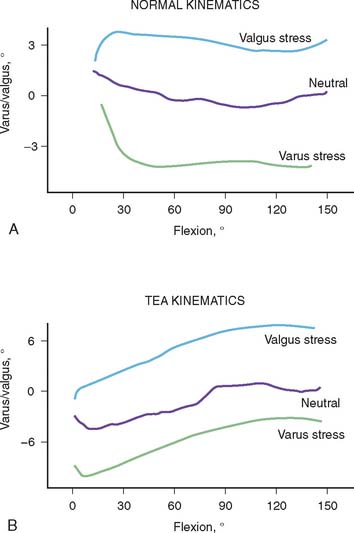
The selection and the rationale for unlinked elbow replacement are described in Chapter 52. The reason for continuing to use a semiconstrained linked implant is simple: the current design works well, is reproducible, and can address a broad spectrum of pathology. The Coonrad-Morrey linked device and similar implants are distinctly different, both conceptually and clinically, from the original, fully constrained articulated devices. In today’s linked prostheses, the one feature in common is that the ulnar component is coupled to the humerus with angular and rotatory laxity of 5 to 10 degrees (Fig. 53-1). The theoretical advantage has been confirmed in the laboratory in which it was demonstrated that the articulation tracks within the limits of its tolerance (Fig. 53-2). This decreases stresses on the bone-cement interface.24 Documentation of improved clinical results attests to the effectiveness of the semiconstrained linked design.2,4,13,14,16,18,21 Of particular note is that the linked implant dramatically broadens the indications for reconstructive surgery of the elbow. Whereas unlinked devices may be very effective for rheumatoid arthritis, the potential for instability limits their use when deformity and osseous and ligamentous deficiency is present. The linked implant may be used with equal effectiveness in patients with rheumatoid arthritis,20 for post-traumatic arthrosis,19 and for revision surgery.18 The enhanced stability supplied by the coupling is provided without transmission of excessive stress to the bone-cement interface with the semiconstrained design.24
CONTRAINDICATIONS
As for any total elbow arthroplasty, the absolute contraindications for a linked arthroplasty are active infection, inadequate soft tissue protection, and the lack of adequate motor muscle power to flex the elbow to ensure proper functioning of the device. Relative contraindications are lack of patient compliance. Primary degenerative joint disease is also a relative contraindication because patients with this disease are usually younger and active, and alternative selections are effective (see Chapter 60). High demand and a dysfunctional hand are also relative contraindications for total elbow arthroplasty.
PRINCIPLES OF SURGICAL TECHNIQUE
SURGICAL INCISION
A straight posterior skin incision is preferred. If a previous incision is present it is employed when possible. If the patient is older than 4 or 5 years of age, it may be repaired if it cannot be incorporated. The incision need not and should not be curved.
THE ULNAR NERVE
Opinions are divided with respect to the management of the ulnar nerve. Some surgeons believe that it should not be exposed,7,9,12,16,27 whereas today most believe that the ulnar nerve should be directly visualized and moved as an integral part of the surgical approach and procedure.4,10,15,23 We favor the latter philosophy.
THE TRICEPS
The fascial tongue exposure of Campbell (Van Gorder) causes a good deal of soft tissue dissection, with a significant amount of dead tissue that provides an environment favorable to infection, which may result in weakness.5,22 Splitting the triceps in the midline is enjoying a resurgence of popularity. In our experience, this tends to cause detachment of the medial insertion. Therefore, I continue to prefer the Mayo technique of reflecting the triceps in continuity with the ulnar periosteum and forearm fascia described by Bryan and Morrey.5 The important point, however, is a meticulous repair (see later).
AXIS OF ROTATION
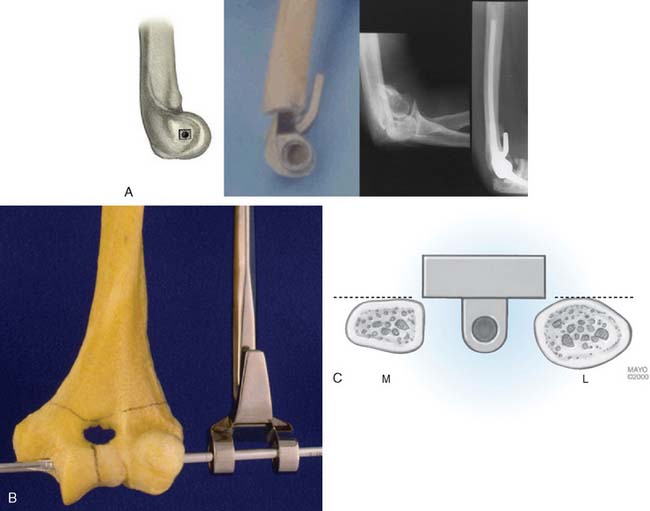
The philosophy of the Coonrad-Morrey device is to use the most reliable landmark to serve as the basis for defining the flexion axis. The landmark selected for this system is the anterior cortex to establish the anterior/posterior position of the axis. The roof of the coronoid fossa is the anatomic reference for depth of insertion, and the plane of the columns define the rotation of the axis of the humeral component (Fig. 53-3).
CEMENTING TECHNIQUE
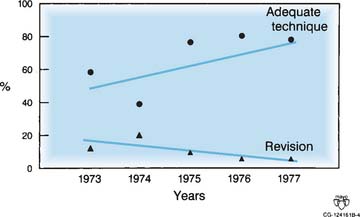
The cement should be introduced down the medullary canal for stemmed implants with an injection system. Generally speaking, injector systems have dramatically improved the radiographic appearance of the bone-cement interface. It was shown in our early experience20,23 and subsequently Faber,8 that the quality of the cementing technique is inversely related to the presence of lucent lines, and, ultimately, to implant loosening (Fig. 53-4).
TRICEPS REATTACHMENT
Triceps reattachment has emerged as a major emphasis for all elbow joint replacement surgery. Whenever the triceps is reflected from its attachment, it must be securely reattached to the olecranon by nonabsorbable sutures placed through bone. The sutures should be tied with the elbow in 90 degrees of flexion, but knots are avoided over the subcutaneous border of the ulna. Because the attachment communicates with the joint and motion will allow the synovial fluid to become interposed between the triceps and the olecranon, an attachment may be compromised. The transverse “cinch” suture applies the tendon to the olecranon. To enhance strength and ensure continuity, we also tend to displace the extensor mechanism slightly medially, if possible, bringing the anconeus slightly over the proximal ulna.
POSTOPERATIVE DRESSING
We have had virtually no incision problems because we have been routinely placing the elbow in full extension with an anterior splint and elevating the arm for approximately 24 hours. We see no advantage to allowing the elbow to assume 90 degrees of flexion immediately after surgery. Because of continued concern for the variable swelling and occasional blistering that may occur after surgery, I no longer use the Steri-Drape, and I avoid Betadine solution if the barrier drape is used. A prospective, randomized study recently revealed statistically measurable decreases in swelling after surgery with the use of a compression Cryocuff (Aircast Co., Coconut Creek, FL).1
THE SEMICONSTRAINED LINKED IMPLANT
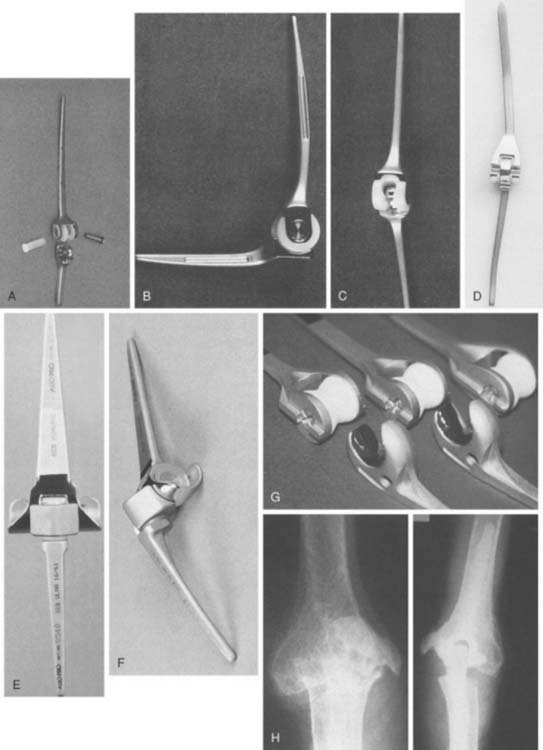
Today, in the United States, several semiconstrained elbow replacements are commercially available, including the Coonrad-Morrey (Zimmer, Warsaw, IN), the Latitude (Tornier, Edina, MN), and the Discovery (Biomet, Warsaw, IN). To date, these two implants have not had sufficient use to document outcomes. The GSB III has evolved through the years and has been frequently used in Europe but its use and support is being discontinued (Fig. 53-5). Experience with the GSB III devices is discussed under the appropriate indications in subsequent chapters. Risung25 has also reported favorable outcomes with a rather novel implant designed termed the Norway elbow.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


