4 Knee Replacement: The Midvastus Approach
Indications
- Total knee replacement
- Revision total knee replacement
- Unicompartmental knee replacement
Contraindications
- Less than 80 degrees of preoperative knee motion
- Obesity
- Hypertrophic arthritis
- Previous high tibial osteotomy
Special Considerations
Advocates of the midvastus approach feel that because the extensor mechanism is not violated, there is less postoperative pain and a faster return of independent knee extension than the medial parapatellar approach. There is also evidence to indicate that it may decrease the number of lateral retinacular releases required for appropriate patellofemoral tracking.
Patient Position
1. Supine on regular operative table
Surgical Procedure
- Anterior, midline skin incision extending from approximately 6 to 8 cm above the patella to the same distance distally just medial to the tibial tubercle
- The fascial layer is opened to expose the medial aspect of the patella and the vastus medialis at its insertion into the quadriceps tendon.
- The prepatellar bursa is opened and reflected medially from the anterior surface of the patella.
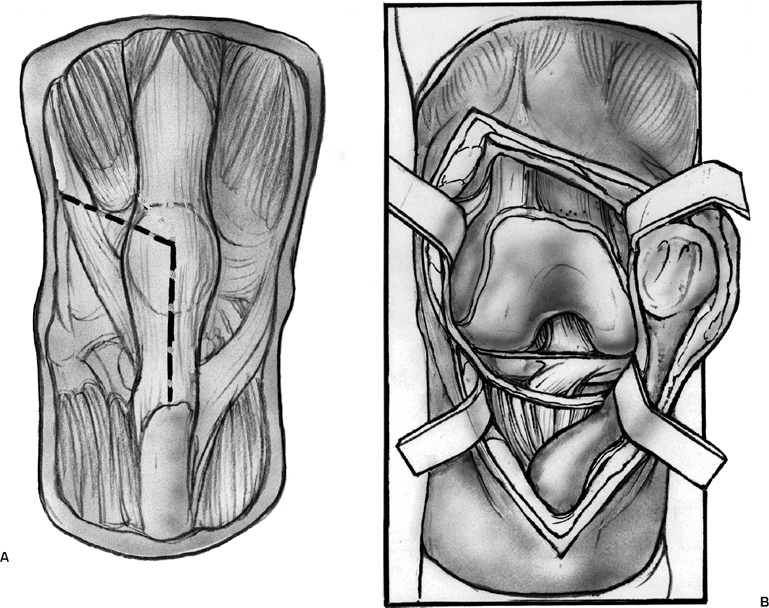
- The vastus medialis muscle is split parallel to its muscle fibers and through the full thickness of the muscle, beginning 4 cm from and extending to the superomedial border of the patella (Fig. 4–1)
- The capsule and retinaculum are opened by sharp dissection along the medial aspect of the patella, leaving a cuff of soft tissue attached to the patella for capsular repair.
- The incision is carried down onto the tibia approximately 1 cm medial to the patellar tendon to the level of the tendon insertion onto the tibial tubercle.
- A subperiosteal layer is elevated from the media tibia to the sagittal midline of the tibia.
- The capsular folds in the suprapatellar pouch are released to allow full eversion of the patella.
- The patellofemoral ligament is cut and a portion of the retropatellar fat pad is removed to allow visualization of the lateral tibial plateau.
- A patellar retractor levering on the tibial plateau helps with full visualization laterally.
- At the conclusion of the procedure a suture is placed at the intersection of the capsular and muscular segments of the incision.
- The capsule and retinaculum are closed with interrupted suture, and the muscle-splitting portion of the approach is not sutured.
Postoperative Care
As outlined in chapter on total knee replacement
Related posts:
 Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
 Total Knee Replacement: Medial Release via Osteotomy
Total Knee Replacement: Medial Release via Osteotomy
 Ligament Advancement in Total Knee Arthroplasty
Ligament Advancement in Total Knee Arthroplasty
 Ligament Injuries: Posterior Cruciate Ligament
Ligament Injuries: Posterior Cruciate Ligament
 Arthroscopic Abrasion Arthroplasty
Arthroscopic Abrasion Arthroplasty
 Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


