Knee
Mark W. Pagnano
GENERAL OBSERVATIONS REGARDING SKIN INCISION
Whenever possible an anterior midline incision should be used for extensive operations that involve the knee joint itself. By extending the skin incision proximally or distally and developing full thickness skin flaps it is possible to reach anterior, medial, and lateral sided structures around the knee. Many patients who require an open operation on the knee as young adults ultimately come to require total knee arthroplasty and the utility of the anterior midline incision should be remembered. If an incision is made medially or laterally it should be far from the midline such that a substantial skin bridge (≥7 cm) is present to accommodate a subsequent anterior midline incision. Rarely today should a surgeon choose to make an oblique or sharply angled incision around the knee as such incisions are difficult to accommodate should future surgery, such as total knee arthroplasty, be required.
STANDARD MEDIAL PARAPATELLAR ARTHROTOMY
Indications
The medial parapatellar arthrotomy has long been the standard arthrotomy for total knee arthroplasty. Modifications of this approach are useful for a variety of procedures including intramedullary nailing of the tibia and articular cartilage transplant.
Position
Supine.
Technique
1. Incision: the extensor mechanism is exposed through an anterior midline incision.
2. The extensor mechanism is exposed both proximally and distally by developing moderate skin flaps. The arthrotomy parallels the medial border of the patellar tendon beginning at the insertion of the pes anserine tendons (Fig. 9-1).
3. The arthrotomy is continued along the medial border of the patella where most surgeons leave a 1 cm sleeve of soft tissue attached to the patella in order to facilitate later closure.
Note: Some surgeons prefer the technique popularized by Insall where the arthrotomy is carried over the medial edge of the patella itself as that approach improves visualization of the medial border of the patella for patellar resurfacing.
The quadriceps tendon is divided for a distance of 8 cm above the superior pole of the patella (Fig. 9-2).
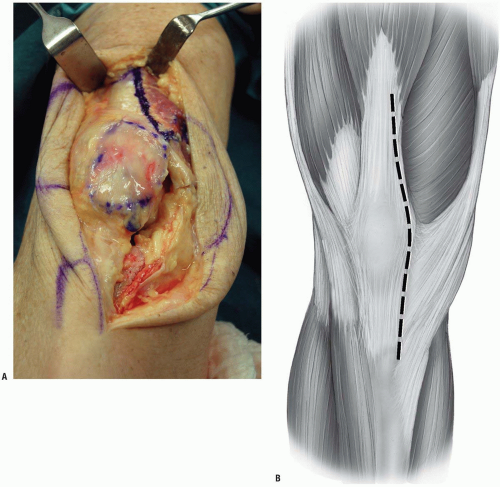 FIGURE 9-1 |
4. Most surgeons leave a small cuff of tendon medially (1 to 2 cm) with the vastus medialis and the great preponderance of the tendon in continuity laterally with the rectus femoris and the vastus lateralis. The retropatellar fat pad is split, the patella is everted, and the knee can be flexed (Fig. 9-3).
Note: An everted patella puts the patellar tendon at risk for avulsion as the tendon is apt to peel from its attachment to the tubercle. If excessive tension is noted in the tendon, the patella should just be subluxed and not everted or the exposure converted to a quadriceps snip.
5. During total knee arthroplasty, a subperiosteal release of the deep portion of the medial collateral ligament can be carried out. As the knee is progressively flexed the tibia can be rotated externally, the anterior cruciate ligament can be excised, and the posteromedial corner of the tibia can be subluxed anterior to the femur (Fig. 9-4).
6. A retractor positioned around the tibial attachment of the posterior cruciate ligament can lever the tibia forward and improve visualization during resection of the proximal tibia (Fig. 9-5).
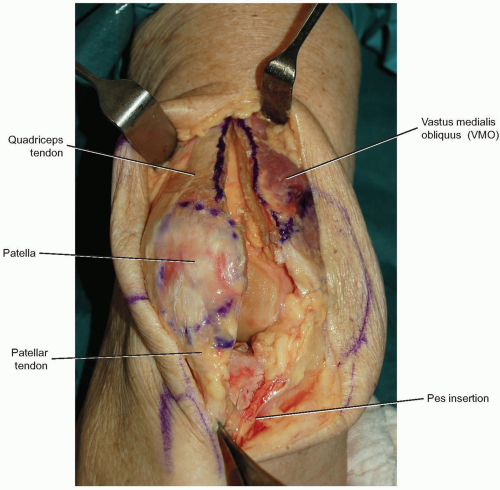 FIGURE 9-2 |
 FIGURE 9-3 |
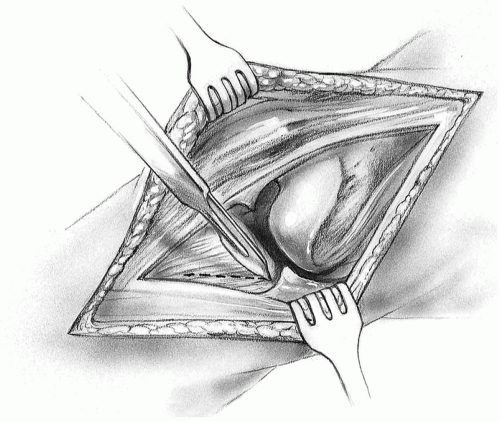 FIGURE 9-4 |
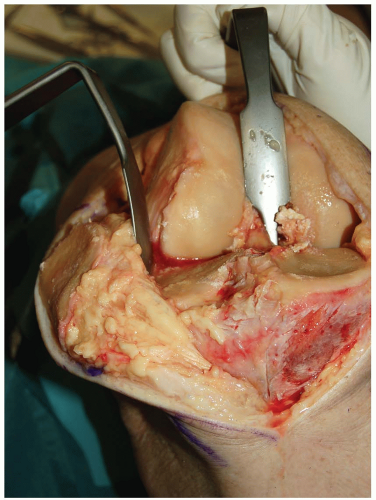 FIGURE 9-5 |
The Quadriceps Snip
In cases where there is excessive tension on the patellar tendon when subluxing or everting the patella, it is useful to perform a proximal quadriceps snip. This approach was introduced by Insall and is particularly useful in knees that are stiff from prior surgery.
A standard medial parapatellar arthrotomy is done.
At the proximal portion of the split in the quadriceps the arthrotomy is then extended proximally and laterally across the remaining extensor mechanism and up into the muscle fibers of the vastus lateralis (Fig. 9-6).
The angle of the cut is the same as the angle of insertion of the vastus lateralis fibers (60 degrees) such that the quadriceps snip can extend itself further into the vastus lateralis if needed (Fig. 9-7).
Note: The quadriceps snip is quite versatile. The vast majority of difficult total knees and revision total knees can be done with a quadriceps snip coupled with adequate debridement of scar tissue from the lateral gutter and around the patella.
The arthrotomy can be closed with multiple interrupted sutures and there is no need to alter the patient’s weight-bearing status after using the quadriceps snip exposure.
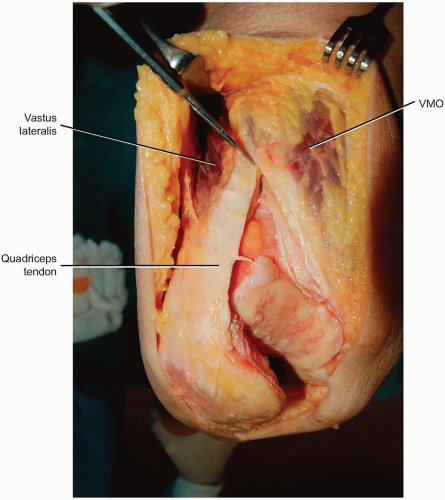 FIGURE 9-6 |
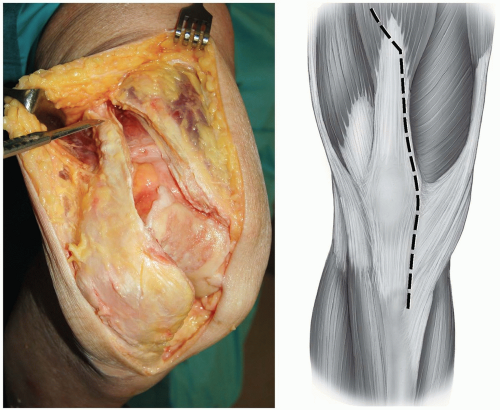 FIGURE 9-7 |
SUBVASTUS APPROACH
Indications
This approach can be used for routine total knee arthroplasty and medial unicompartmental knee arthroplasty.
Because it preserves the entire extensor mechanism’s attachment on the patella, the subvastus approach has an anatomic edge on other arthrotomies of the knee joint. Recent anatomic studies at the Mayo Clinic have confirmed that the tendon of the vastus medialis extends all the way to the midpole of the patella. Thus any arthrotomy that extends proximal to the midpole disrupts part of the extensor mechanism.
Technique
Incision: the standard subvastus approach is done through a midline incision.
Care is taken to develop a medial skin flap to truly define the inferior border of the vastus medialis obliquus (VMO) (Fig. 9-8).
Note: The VMO attaches to the patella at a 50 degree angle and always extends more distally and more medially than the surgeon is inclined to think. The subvastus arthrotomy is made by incising the retinaculum and joint capsule at the VMO muscle edge from proximal to distal at the same 50 degree angle as the VMO itself. Care should be taken to extend the arthrotomy to the midpole of the patella and not to cheat the arthrotomy up toward the superior pole of the patella.
At the midpole of the patella the arthrotomy is turned distally and parallels the medial border of the patellar tendon (Fig. 9-9).
The fat pad is split and the patella can be subluxed into the lateral gutter of the knee. In cases where the patella is difficult to sublux laterally, the surgeon will usually find a tight band of tissue proximal-medially (the medial patellofemoral ligament) that must be released. Once the medial patellofemoral ligament is released the patella will sublux laterally with relatively little force (Fig. 9-10).
If desired the patella can be everted at this stage and the knee flexed (Fig. 9-11).
Note: Everting the patella is difficult in heavily muscled patients and markedly obese patients. In those patients the patella should just be subluxed into the lateral gutter. In patients with substantial patella baja the subvastus approach is not recommended.
When closing the subvastus arthrotomy it is useful to tension and tie the capsular sutures with the knee in 90 degrees of flexion to avoid overtightening the medial capsule.
 FIGURE 9-8 |
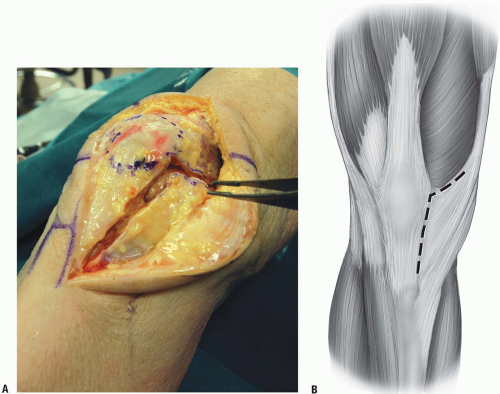 FIGURE 9-9 |
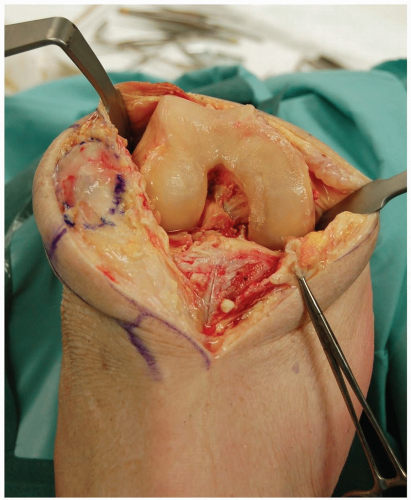 FIGURE 9-10 |
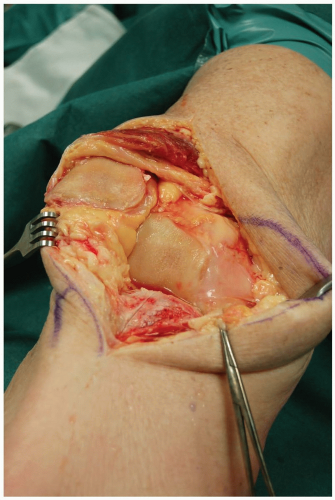 FIGURE 9-11 |
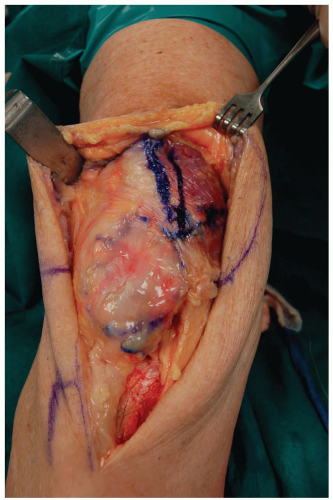 FIGURE 9-12 |
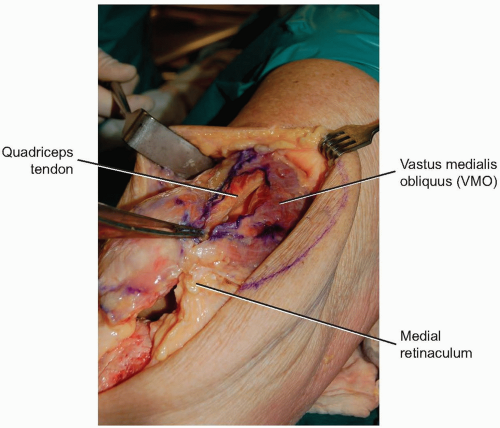 FIGURE 9-13 |
TRIVECTOR RETAINING APPROACH
The trivector approach can be used for total knee and medial unicompartmental knee arthroplasty.
Technique
Incision: an anterior midline incision is made and the vastus medialis muscle and tendon are identified.
The knee is flexed to 90 degrees and, beginning three finger-breadths proximal to the patella, the arthrotomy is made from proximal to distal 2 cm medial to the quadriceps tendon (Fig. 9-12).
This means the arthrotomy involves transection vastus medialis muscle fibers proximal and medial to the patella (Fig. 9-13).
The arthrotomy is extended distally along the medial border of the patella and the medial edge of the patellar tendon. The fat pad is split, the patella is everted with the knee in extension, and then the knee can again be flexed.
At the time of closure the surgeon will see that the edge of the quadriceps tendon actually extends medially under the cut muscle fibers of the vastus medialis. Thus there is reasonable tissue through which to place sutures and close the joint itself.
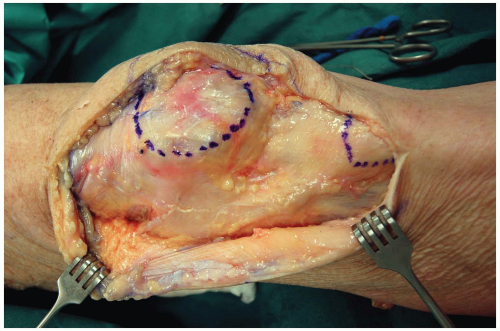 FIGURE 9-14 |
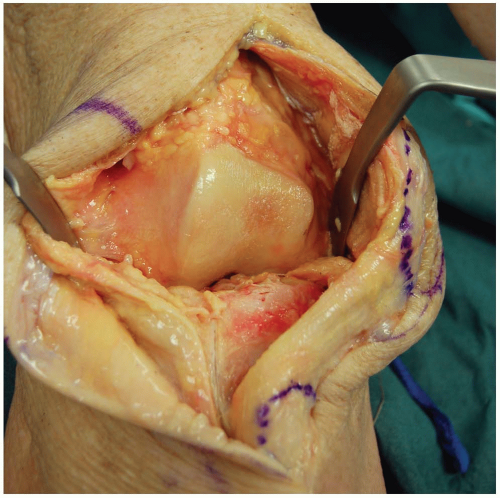 FIGURE 9-15 |
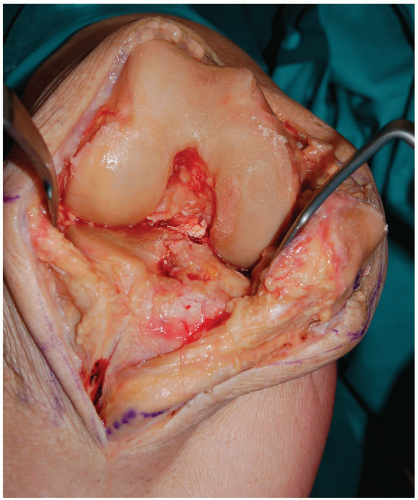 FIGURE 9-16 |
LATERAL APPROACH FOR TOTAL KNEE ARTHROPLASTY IN THE VALGUS KNEE
Indications
For patients with substantial valgus deformity who require total knee arthroplasty some surgeons use an anterolateral approach.
Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


