Forearm
Bernard F. Morrey
POSTERIOR APPROACH TO THE RADIUS (THOMPSON)
Indications
Fracture, tumor, and infection when access to posterior radius desired.
Note
This approach is not commonly employed but may be used to expose either the proximal, mid or distal radius but is most effective for the proximal and middle thirds.
Position
The patient is supine with arm across the chest or on arm/elbow table.
Landmarks
Lateral epicondyle to radial styloid.
Technique
1. Incision: straight from the lateral epicondyle to the radial styloid. With the forearm pronated the line of the incision is a straight line. Use all or any portion (Fig. 2-1A).
2. Expose the interval between the anterior border of the extensor digitorum communis and the posterior or radial border of the extensor carpi radialis brevis.
3. Distally palpate the bare portion of the radius distally that superficially demarcates the natural interval between these two muscle groups (Fig. 2-1B). Deep to these muscles the bare area identifies the distal aspect of the supinator and proximal attachment of the pronator teres tendon.
4. The forearm fascia is split proximally and distally allowing the extensor digitorum communis to be retracted posteriorly and extensor carpi radialis brevis to be retracted anteriorly to the ulnar side of the radius (Fig. 2-1C). The bare shaft of the radius between the supinator and pronator attachments is well defined (Fig. 2-1D).
5. Proximally with the forearm in supination, the supinator muscle is noted and the posterior interosseous nerve observed and may or may not be exposed.
6. The supinator muscle is then released either in its mid-portion exposing the posterior interosseous nerve or, more commonly, is released from the shaft of the radius (Fig. 2-1E).
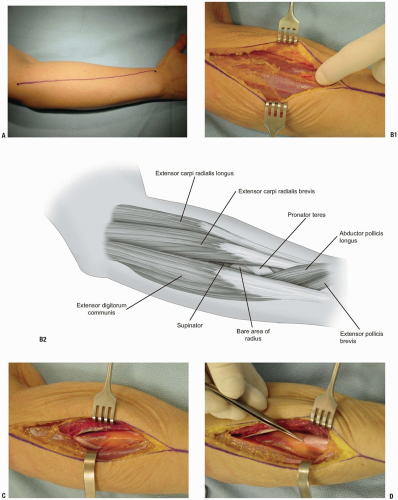 FIGURE 2-1 |
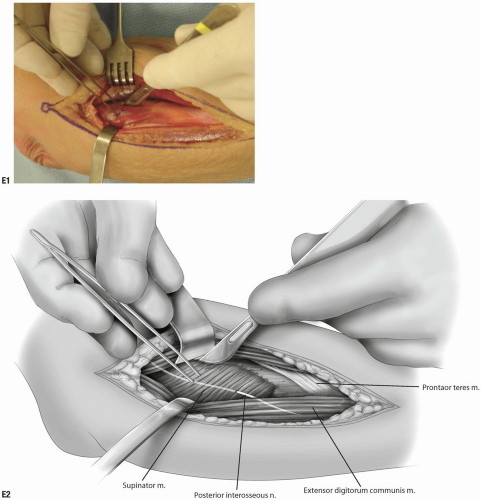 FIGURE 2-1 (Continued) |
• Pearls
This is facilitated by fully supinating the forearm which brings the supinator attachment of the radius easily within the wound allowing excellent visualization for the release of its origin.
It is not necessary to identify the posterior interosseous nerve during this procedure but one should be gentle to avoid nerve injury.
7. The supinator muscle is reflected towards its ulnar attachment and the proximal portion of the radius is exposed (Fig. 2-1F).
8. After splitting the forearm fascia distally, the common extensor is reflected posteriorly and the tendinous portion of the brevis and longus is isolated in the midforearm (Fig. 2-1G). The radial attachment of the pronator teres muscle is in the mid-portion of the exposure.
9. Distally, by retracting the extensor digitorum communis posteriorly and extensor carpi radialis brevis anteriorly, the abductor pollicis longus and extensor polis brevis are observed to course obliquely superficial to the extensor carpi radialis brevis tendon at the distal aspect of the incision (Fig. 2-1H). The middle 80% of the radius is exposed.
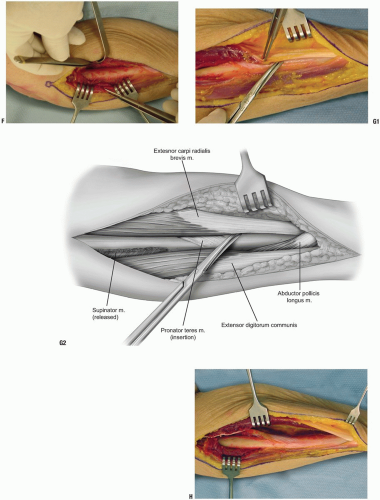 FIGURE 2-1 (Continued) |
ANTERIOR (HENRY) SURGICAL EXPOSURE TO THE PROXIMAL RADIUS
Indications
Fracture, malignancy, and osteomyelitis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


