Elbow
Bernard F. Morrey
Facility with exposures to the elbow characterized by flexibility and extensibility is an essential prerequisite to the execution of the full spectrum of elbow surgery which is discussed in detail in Master Techniques in Orthopedic Surgery: The Elbow (1). In this chapter we emphasize how limited exposures to the elbow can be expanded to address broadened pathology and perform more complex procedures. Specific details of exposure and technique are found in the above cited volume.
There are two conceptual incision types: an extensile posterior or posterior/lateral or a limited, specific for-purpose exposure (Fig. 3-1). For extensile exposures, a straight posterior or posterior lateral incision is used. We term the posterior exposure the “universal” incision since both medial and lateral elbow pathology can be addressed through a posterior skin incision by elevating skin flaps (Fig. 3-2). For fear of injuring the ulnar nerve, a posterior incision of variable length (12 to 18 cm) is placed just medial or lateral to the tip of the olecranon and not directly over the cubital tunnel.
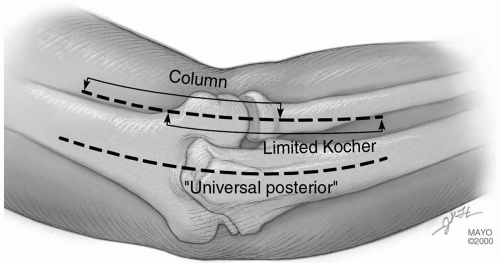 FIGURE 3-1 |
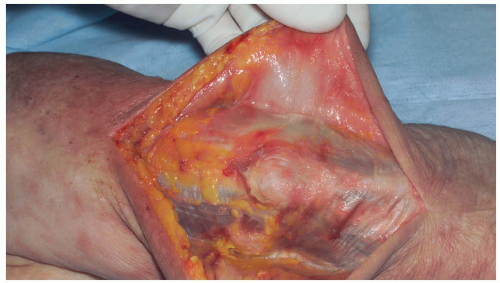 FIGURE 3-2 |
OLECRANON OSTEOTOMY
Indications
Reduction and fixation, distal humeral, and comminuted fractures (C3).
Landmarks
Tip of olecranon, medial epicondyle, ulnar nerve in cubital tunnel, nonarticular portion of olecranon.
Position
The patient is supine with arm across the chest.
Technique
Skin incision: direct posterior from 6 to 8 cm proximal to the tip of the olecranon, over subcutaneous border of ulna; distal as required (Fig. 3-3A).
Elevate skin flaps medially and laterally to the epicondyles (Fig. 3-3B).
Identify ulnar nerve and incise medial ulnohumeral capsule.
The anconeus is released from the triceps, the ulnohumeral capsule is incised, and the nonarticular portion of the greater sigmoid notch is identified (Fig. 3-3C).
Alternate: Laterally, we prefer to protect and elevate the anconeus distal to proximal thereby protecting its origin from the triceps fascia (see later).
A Chevron osteotomy is performed, apex distal with a depth of 5 to 10 mm (Fig. 3-3D). Protect the ulnar nerve medially. Use osteotome to crack last few millimeters to assure accurate subsequent reduction.
The olecranon fragment is reflected proximally exposing the distal humerus (Fig. 3-3E).
Repair uses the AO-K-wire, tension band technique with the wires in the anterior cortex, not down the canal (Fig. 3-3F).
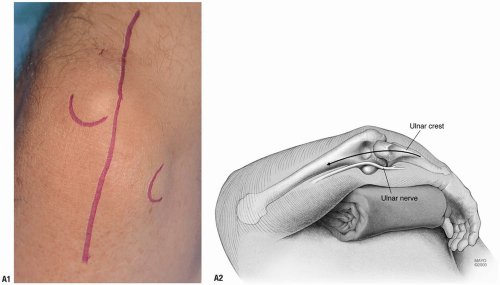 FIGURE 3-3 |
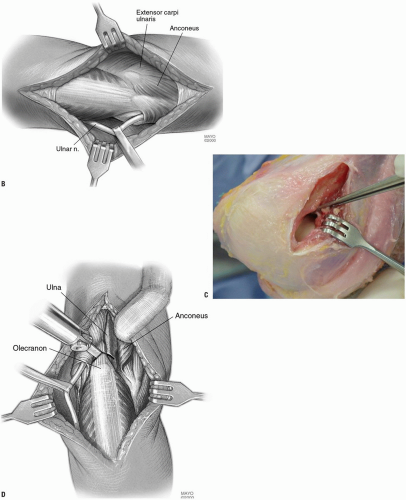 FIGURE 3-3 (Continued) |
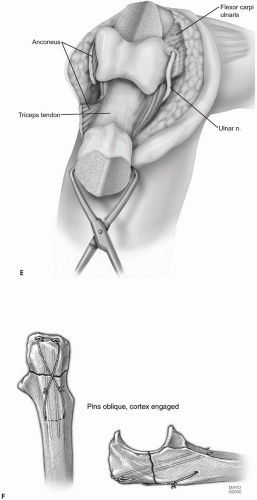 FIGURE 3-3 (Continued) |
Mayo Olecranon Osteotomy of the Elbow—Anconeus Preserving
Concern with regard to transecting the anconeus attachment to the triceps has prompted the development of an olecranon osteotomy that preserves the anconeus origin and viability.
Position
The patient is supine with the arm across the chest.
Technique
The exposure is as required by the pathology. Deep exposure is at the Kocher’s interval between the extensor carpi ulnaris and anconeus (Fig. 3-4A).
The interval is entered and the anconeus is identified and isolated (Fig. 3-4B).
The anconeus is elevated from its bed by sharp dissection leaving the attachment of its origin at the fascial expansion of the triceps and the mid-portion of the sigmoid notch is identified laterally (Fig. 3-4C).
Medially the ulnar nerve is identified (Fig. 3-4D) and the mid-portion of the articulation is exposed (Fig. 3-4E).
A V-shaped osteotomy is carried out as above with an oscillating saw (Fig. 3-4F). The osteotomy is completed with an osteotome (Fig. 3-4G).
The osteotomized olecranon along with the attached anconeus is elevated proximally (Fig. 3-4H).
Closure consists of the standard AO reattachment of the olecranon. The anconeus is brought back to its insertion on the ulna. The fascia over the anconeus is closed with a running 2-0 absorbable suture (Fig. 3-4I).
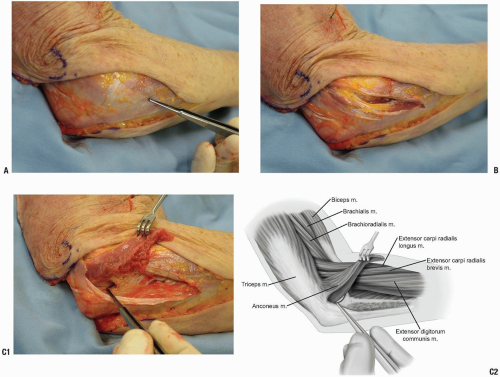 FIGURE 3-4 |
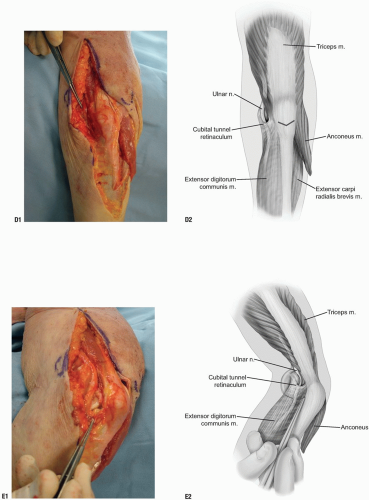 FIGURE 3-4 (Continued) |
 FIGURE 3-4 (Continued) |
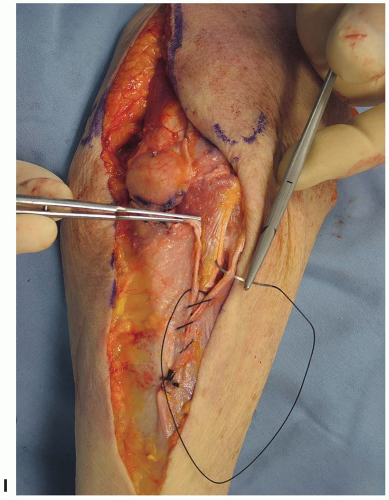 FIGURE 3-4 (Continued) |
Pearls/Pitfalls/Comments
Pearl: The ulnar nerve does not need to be mobilized unless dictated by the pathology.
Comments: The attractiveness of this exposure is that the anconeus dissection can be done very safely and quickly. This does preserve the anconeus triceps continuity in the event that a later reconstructive procedure may be necessary that uses the anconeus.
Pitfalls: Avoid osteotomy in rheumatoid arthritis as the thin olecranon compromises healing if an osteotomy is carried out (2). The transverse osteotomy of McAusland is associated with an approximately 5% nonunion rate (2). Although for fractures the Chevron osteotomy may improve these results and decrease the nonunion rate, I personally have not had the clinical need to osteotomize the olecranon in the last 14 years, and osteotomy should be avoided if the olecranon is resorbed.
LATERAL EXPOSURES
The central concept is predicated on raising subcutaneous flaps both medially and laterally. This in turn is strongly dependent on recognizing the flexibility of extending limited incisions as needed.
A limited proximal lateral approach exposes the supracondylar column. A limited distal approach enters Kocher’s interval and exposes the radial head and the lateral collateral ligament. Connecting the two defines the extensile Kocher exposure (Fig. 3-5).
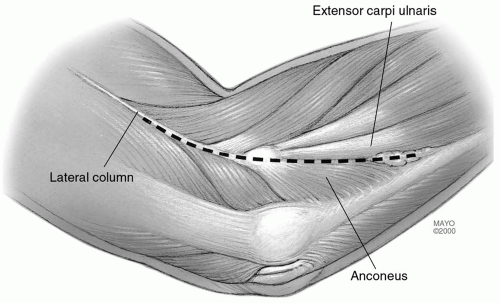 FIGURE 3-5 |
The Column Exposure (3)
Indications
Anterior-posterior capsular release for stiff elbow.
Landmarks
Lateral epicondyle, the common extensor tendon, the extensor carpi radialis longus, and the anterior capsule.
Position
The patient is supine with arm across the chest.
Technique
Incision: the skin incision starts over the lateral column 5 cm proximal to the lateral epicondyle and extends distally 2 cm past the epicondyle (Fig. 3-6A).
The extensor carpi radialis longus is identified and elevated from the lateral column and epicondyle and the anterior capsule is visualized (Fig. 3-6B).
An incision is made in the capsule just superior to the collateral ligament (Fig. 3-6C).
If the posterior joint needs to be exposed the triceps is easily elevated (Fig. 3-6D).
 FIGURE 3-6 |
 FIGURE 3-6 (Continued) |
Pearls/Pitfalls/Comments
A periosteal elevator is used to elevate the brachialis muscle off the anterior capsule which can be safely performed since the arthrotomy provides accurate spatial orientation from lateral to medial across the joint.
Special contoured retractors have been designed making the soft tissue retractor easier (Fig. 3-6E).
If an extensile exposure is anticipated, a posterior incision is made. The same deep exposure can be accomplished by extending the posterior lateral skin incision and elevating the lateral skin cutaneous flap.
Limited Kocher Exposure of the Elbow
Indications
Simple excision of the radial head and repair of lateral ulnar collateral ligament.
Landmarks
Lateral epicondyle, radial head, and interval between anconeus and extensor carpi ulnaris.
Position
The patient is supine with arm across the chest.
Technique
Incision: from the subcutaneous border of the ulna obliquely across the posterolateral aspect of the elbow ending just proximal to the lateral epicondyle (Fig. 3-7A).
Note: This follows Kocher’s interval.
The interval between the anconeus and extensor carpi ulnaris is identified and entered (Fig. 3-7B).
For excision of the radial head, the extensor carpi ulnaris and a small portion of the supinator muscle are dissected free of the capsule and retracted anteriorly (Fig. 3-7C).
 FIGURE 3-7 |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


