Cervical Spine
Robert K. Eastlack
Bradford L. Currier
The complex and often variable anatomy of the cervical spine mandates careful preoperative planning and an appreciation of the limitations inherent in each surgical approach. Such planning can significantly reduce the technical demands of the surgery, and reduce the likelihood of complications.
With all of the approaches, optimizing patient positioning prior to an incision will lead to a smoother procedure, and may improve the result of the operation. This includes the use of imaging modalities after positioning to ensure adequacy of the image, which can be adjusted much more easily prior to final preparation and draping of the patient.
Indications for a particular approach depend largely on the anatomic levels requiring surgical management, as well as the techniques planned for any reconstruction. Table 12-1 lists the more common anterior and posterior approaches, and the cervical levels exposed most effectively by each approach. With the advent of fluoroscopically guided techniques (i.e., transarticular C1-2 screws or anterior odontoid screws), one must also consider the trajectories required for placing instrumentation when choosing the surgical approach.
ANTERIOR APPROACHES
Transoral Approach
Indications
This approach is typically used for resection of anterior processes, such as the odontoid with basilar invagination, infection, tumors, irreducible odontoid fractures in chronic dislocations, and congenital disorders of the anterior axis or atlas.
As its name implies, this approach uses the oral cavity as its pathway to the upper cervical spine. Visualization can be difficult due to the constraints of the jaw and oral cavity, but it can allow direct access from the clivus to the upper portion of C3. Although there is little vascularity encountered when approaching the spine through this midline approach, infection and cerebrospinal fluid leakage have been considerable problems in the past. The heightened chance of infection and historically poor outcome of bone grafting with the transoral approach make it a questionable choice for use during
anterior cervical fusions (1). The limitations in exposure with this approach can be reduced by the use of mandibular osteotomies. Morbidity from these techniques can be substantial; however, the approach does allow unique anterior exposure from the clivus to C6. It is typically useful for lesions within the bodies of C2-3, and when the oral cavity cannot be easily traversed, such as with severe temporomandibular joint arthrosis or an interdental distance less than 25 mm.
anterior cervical fusions (1). The limitations in exposure with this approach can be reduced by the use of mandibular osteotomies. Morbidity from these techniques can be substantial; however, the approach does allow unique anterior exposure from the clivus to C6. It is typically useful for lesions within the bodies of C2-3, and when the oral cavity cannot be easily traversed, such as with severe temporomandibular joint arthrosis or an interdental distance less than 25 mm.
TABLE 12-1. Common Approaches to the Cervical Spine | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Preoperative Planning/Preparation
As with all spine surgery, medical comor-bidities should be ascertained, but particular focus must be paid to nutritional status. Total lymphocyte count and albumin are generally useful markers of nutritional status. Dental evaluations should be performed preoperatively to ensure an oral cavity that is free from ongoing infection. Standard preoperative antibiotic recommendations currently include an intravenous cephalosporin and metronidazole.
Position
A padded headrest or Gardner-WellsTM tongs are used to stabilize the head with the patient in the supine position. Awake, nasotracheal intubation may be performed with or without fiberoptic assistance depending on the perceived stability of the cervical spine. Once a neurologic examination is performed, anesthetic can be administered, and then the patient can be placed in a mild reverse-Trendelenberg position to prevent aspiration (2). Various retractors can be used for widening the interdental gap, such as the Codman Crawford or the Spetzler-Sonntag transoral retractors (Figs. 12-1, 12-2 and 12-3). The soft palate can often be elevated with a malleable self-retainer. Alternatively, two Red Robin catheters can be fed through the nares (one on each side) and brought out through the mouth. Once both catheters have been placed, the two ends on each side are tensioned superolaterally and secured to the drapes. Prepare the oropharyngeal area with betadine solution, and place a throat packing to prevent debris from falling into dependent laryngeal spaces or the trachea. Obtain localizing radiographs once the posterior pharyngeal area is exposed, and then inject epinephrine solution along the site of planned incision. Although surgical loupes with overhead illumination can be used in these cases, an operating microscope provides a clearer image and allows for easier assistant participation.
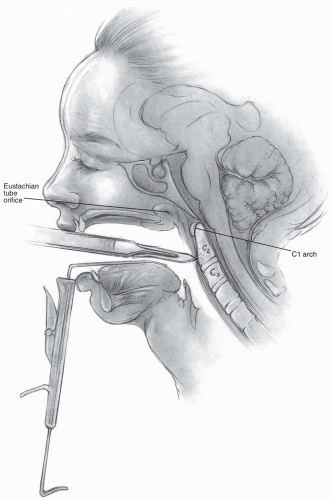 FIGURE 12-1 |
 FIGURE 12-2 |
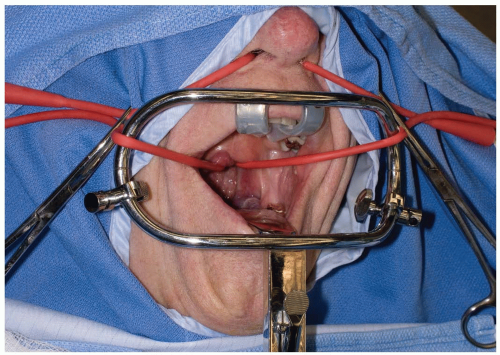 FIGURE 12-3 |
Landmarks
The tubercle of the atlas can be palpated to discern the midline, and a vertical incision is carried out 1 to 2 cm above and below the tubercle in the midline (Fig. 12-4).
Technique
Incision: the incision is made full thickness to bone through the mucosa and pharyngeal musculature. Subperiosteal elevation should be carried out from the midline, which will bring the longus colli muscles and anterior longitudinal ligaments laterally. Lateral elevation on the atlas should be restricted to 1.5 cm from the midline, as the vertebral arteries, internal carotid arteries, and hypoglossal nerves are at risk with more aggressive lateral exposure (3) (Fig. 12-5). The internal carotid artery can be quite close to the midline, as suggested by Currier et al, who found it more than 7.5 mm medial to the foramen transversarium in 6% of their subjects (4). The hypoglossal nerve lies approximately 2 to 3 mm lateral to the middle of the anterior aspect of the C1 lateral mass (5) (see Fig. 12-5).
If access to the odontoid is desired, the central 1 to 1.5 cm of the atlas may be resected to expose the upper portion of C2. Should the anterior portion of the atlas be removed, attempt to preserve the transverse ligament, if possible. The transverse ligament prevents lateral displacement of the atlas lateral masses, which can lead to craniocervical instability (6). If it cannot be preserved, a posterior occipitocervical arthrodesis may be necessary. Soft tissues, such as pannus, can be resected from the areas surrounding the bony anatomy, but residual amounts adherent to the dura may best be left in place to avoid cerebrospinal fluid (CSF) leakage. The tectorial membrane can be decompressed to allow improvement in CSF flow.
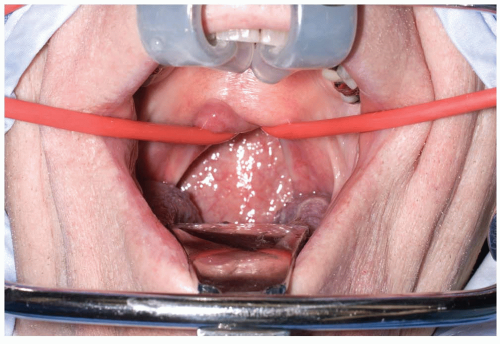 FIGURE 12-4 |
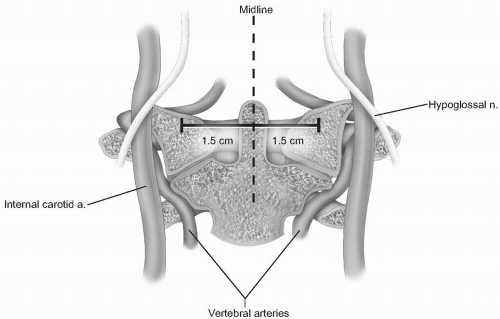 FIGURE 12-5 |
Postoperative Management
Once the resection portion of the procedure has been completed, CSF containment should be confirmed with a Valsalva maneuver, and then reconstruction or closure can proceed. If possible, the longus colli is reapproximated in the midline, followed by absorbable suture approximation of the pharyngeal layer. Intubation is typically continued for 1 to 2 days due to the risk of swelling postoperatively. Antibiotic regimens vary in the literature, but we typically use cefazolin and metronidazole for 5 to 7 days starting immediately preoperatively. The metronidazole can be administered through a nasogastric feeding tube placed intraoperatively after wound closure. Clear liquids are begun approximately one week after surgery, but a regular diet should be withheld until 3 weeks postoperatively (6).
Complications
Rates of complication with the transoral approach have been quoted between 18% and 26%, including a mortality rate of 6%, according to one source (7). Although early use of the approach led to very high infection rates (above 50%), more recent studies demonstrate infection rates below 3% (8, 9, 10). CSF leakage during the procedure should be addressed with attempted closure, grafting, fibrin glue, and a meticulous closure, as the persistence of leakage can result in fistula formation (11). A lumbar drain should be strongly considered in this situation, as the persistence of CSF leakage can be exceptionally troublesome. Other potential complications include bleeding from injury to the vertebral or internal carotid arteries, craniocervical instability, lingual swelling, and postoperative infection.
Anterior Retropharyngeal Approach
Indications
The high retropharyngeal approaches allow access to the anterior upper cervical spine, and may be indicated for debridement of tumors or infection, and stabilization of the atlantoaxial segment. It is possible to expose the C1-2 facet articulations at the upper end of the approach, while the most caudal access afforded by the primary incision is the upper end of C3. An extensile vertical incision can be employed to allow access to the mid and lower cervical regions.
Although this approach can be carried out medial (anterior approach) or lateral (anterolateral approach) to the carotid sheath, we favor the use of the method described by McAfee and colleagues, termed the anterior retropharyngeal approach (12). It is an extension of the Southwick and Robinson approach initially described for use in the lower cervical spine (13). By accessing the retropharyngeal space medial to the carotid sheath, one avoids the risk of injuring the carotid vessels or cranial nerves at the skull base, but there is a higher risk of injury to the superior laryngeal or glossopharyngeal nerves than when approached lateral to the carotid sheath. Additionally, the anterior approach allows access to both vertebral arteries, while exposing lateral to the carotid sheath compromises access to the contralateral vertebral artery. Finally, anterior decompression and reconstructive measures may be more easily performed when visualizing the spine from the anterior approach than the anterolateral approach.
Preoperative Planning/Preparation
Particular attention should be focused on any compromise of swallowing or respiratory function. In the revision setting, it may be necessary to have the patient undergo vocal cord evaluation. A preoperative tracheostomy may be warranted to avoid airway problems, and an otolaryngologist can assist with this determination. When attempting tumor resections, angiography or a CT angiogram should be obtained to define the locations of the vertebral arteries.
Position
The patient is placed in a supine position, and cranial traction should be strongly considered. If postoperative halo-vest immobilization is planned, the use of a halo ring can be substituted for Gardner-Wells tongs. Before traction is applied, baseline evoked potentials from neuromonitoring should be obtained (if used). The patient should be awake for fiberoptic nasotracheal intubation, so neurologic assessment can be performed following the intubation and positioning. Oral placement of tubes or devices should be avoided, as they may inferiorly displace the mandible and compromise maximum exposure of the upper-most aspects of the cervical spine. Finally, place the patient in a slight reverse-Trendelenberg position to aid in visualization and improve venous drainage.
Landmarks
Unlike lower areas of the cervical spine, the side of approach need not be dictated by underlying anatomical variations. A right-sided approach may be easier for those surgeons with right-handed dominance, but if there is a foreseeable need to extend below C5 then one should consider a left-sided approach to avoid injury to the recurrent laryngeal nerve. Tumor location predominantly on one side may also influence the need for approach on a particular side. Mild head rotation can facilitate the exposure. If performing the anterolateral high retropharyngeal approach, the ipsilateral earlobe should be prepped and then sutured to the cheek anteriorly. Otherwise, it will be an obstruction during the exposure.
Technique
Incision: the submandibular incision for the anterior approach begins at the tip of the mastoid process and traverses medially to the level of the hyoid bone (modified Schobinger incision) (14). When more caudal exposure is desirable a vertical incision can be made along the sternocleidomastoid to intercept the submandibular incision (Figs. 12-6 and 12-7). Once the superficial fascia and platysma are divided, skin flaps can be raised deep to the platysma. Before proceeding more deeply, a nerve stimulator can be used to find the mandibular branch of the facial nerve (Fig. 12-8). It generally courses superiorly above the retromandibular vein and should be preserved due to its innervation of the orbicularis oris muscle. The retromandibular vein can be sacrificed by ligation adjacent to its junction with the internal jugular vein.
The facial vein can be found and ligated just inferior to the submandibular gland (Fig. 12-9). It typically courses superficial to the gland and is oriented cephalocaudally. By leaving the ligature on the superior stump of the vein, it can be used to retract the superficial fascia of the submandibular gland and protect the marginal branch of the mandibular nerve as it courses within the fascia. The submandibular gland is then mobilized superiorly, exposing the intersection of digastric and stylohyoid muscles. These muscles are divided at their confluence near the hyoid bone and reflected proximally (Fig. 12-10). Occasionally, the submandibular gland must be resected to allow adequate exposure; however, its corresponding salivary duct must then be ligated to prevent fistula formation.
Next, the superior thyroid, lingual, and facial arteries and associated veins are ligated and divided (Fig. 12-11). It is helpful to proceed from inferior to superior during this process, using the hyoid bone as a marker for localizing each artery. The superior thyroid artery is just below the hyoid bone, while the lingual and facial arteries are at and just above it, respectively. The superior laryngeal nerve often travels close to the superior thyroid artery, and injury to it must be avoided.
The deep fascia can now be divided along the border of the sternocleidomastoid muscle, and the carotid sheath is localized by palpating the internal carotid pulse. Once the digastric and stylohyoid muscles have been transected, the hyoid bone and accompanying pharyngeal structures can be more easily mobilized medially. Care should be taken not to retract these muscles too vigorously near the mastoid, as the facial nerve courses through this area and may sustain a neuropraxic injury.
The hypoglossal nerve is found more superior than the superior laryngeal nerve; both should be protected by careful dissection and mobilization. Once the hypoglossal nerve is dissected out from its exiting site at the skull base to its insertion near the tongue, it can be retracted superiorly (Fig. 12-12, see Fig. 12-10B). The carotid sheath can then be retracted posterolaterally. Although medial retraction of the pharynx is helpful, excessive force can cause iatrogenic injury to the laryngeal and pharyngeal branches of the vagus nerve. Use blunt finger dissection to separate the carotid sheath from the medial pharynx and larynx, and the retropharyngeal space can then be safely entered.
A peanut or Kittner dissector can now be used to clear alar and prevertebral fascia away from the longus colli muscle, which is then divided longitudinally in the midline (Fig. 12-13). The longus colli muscles insert on the anterior arch of the atlas bilaterally, so they can help define the midline of C1 if adequately exposed. When starting the midline incision, avoid extending beyond the cephalad margin of the atlas, which could violate the anterior occipitoatlantal membrane. The incision is carried down to bone and subperiosteal flaps are elevated laterally. The anterior longitudinal ligament underlying the longus colli should be reflected within these flaps. Limit lateral elevation of these flaps on the atlas to 1.5 cm from midline, as the vertebral arteries can be in significant danger beyond this distance.
If decompression is planned, it should generally be performed in a cephalad-to-caudal direction. This reduces difficulty with visualization, as bleeding tends to run in a caudal direction. The posterior longitudinal ligament and uncovertebral joints help identify the posterior and lateral safety margins of the decompression. If reconstruction is to be performed, the head should be carefully repositioned to neutral alignment prior to graft placement and fixation.
The transected digastric and stylohyoid muscles should be reapproximated with sutures. Similarly, the origin of the sternocleidomastoid muscle must be repaired at the mastoid process. Before occlusion of the retropharyngeal space, a drain should be placed in this deeper area of the wound. The platysma can be reapproximated with a running absorbable suture, followed by the skin in a routine fashion according to the surgeon’s preference.
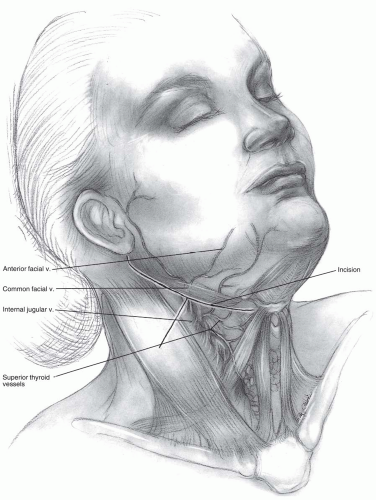 FIGURE 12-6 |
 FIGURE 12-7 |
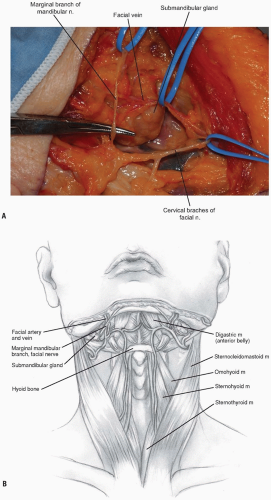 FIGURE 12-8 |
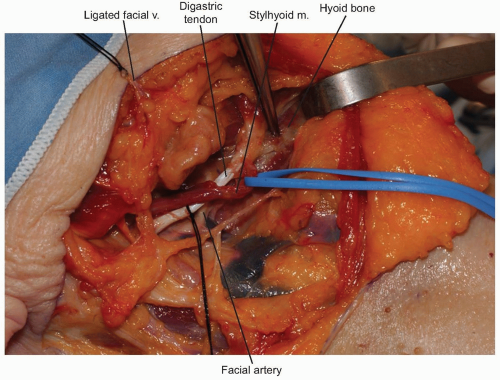 FIGURE 12-9 |
 FIGURE 12-10 |
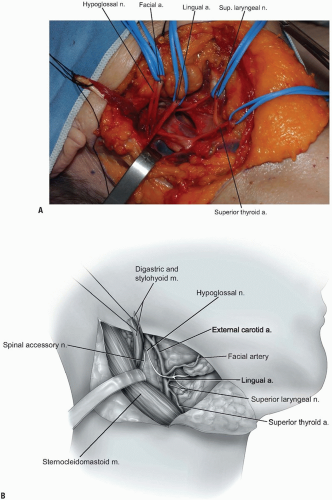 FIGURE 12-11 |
Postoperative Management
Extubation may be performed immediately after surgery, but longer cases or those with greater likelihood of significant edema should be considered for a day or two of continued intubation. Less commonly, tracheostomy might be required immediately or in a delayed fashion if there is more serious airway compromise or concern. Drains are typically left in for approximately 24 hours, but higher outputs may necessitate longer durations or exploration in cases of persistent heavy bleeding. It is generally advised to keep the head of the bed elevated to encourage more rapid resolution of edema. Dietary advancement should begin with sips of water or clear liquids, and then slow progression may ensue if tolerated on the first postoperative day.
Complications
Neurapraxias or lacerations of various nerves may occur during the high retropharyngeal exposures. Injury to the mandibular branch of the facial nerve may cause drooping of the ipsilateral mouth corner, but this usually resolves spontaneously over the first few postoperative months in cases of neuropraxia. The hypoglossal nerve typically recovers from neuropraxic injury within several months after surgery (6Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



