1 Introduction
Vibration training and vibration therapy, also known as whole body vibration (WBV), biomechanical stimulation (BMS), and biomechanical oscillation (BMO) date back to ancient Greece. Recently, vibration training has been reinvented as a new form of exercise that is becoming more frequently used to improve muscle strength, power and flexibility as well as coordination. Increasingly, WBV can be encountered in different wellness, fitness and rehabilitation centres as well as medical centres. Various professional sports clubs, such as AC Milan (soccer), Anaheim Mighty Ducks (ice hockey) and Chicago White Sox (baseball), are using WBV for their recovery and strengthening regimens in addition to their warm-up sessions. Individual professional athletes, including the legendary cyclist Lance Armstrong and Austrian skiing star Herman Maier, have incorporated vibration platform sessions into their training schedules.
Initially, vibration was used only for specific parts of the body (BMS). Later, a system with a counter movement (lateral or horizontal displacement) around a fulcrum was licensed in Germany, in 1996. Individuals using this tool could stand on their feet so that the whole body was stimulated with a sinusoidal vibration; hence the term whole body vibration was coined. This should not be confused with the vibration experienced in occupational injuries where the body passively vibrates over long periods of time. In the latter case, occupational vibration differs in its duration (e.g. heavy machinery driver) and also in the nature of its form, whereby sporadic movements are induced in the body, as in an air compression hammer, at a totally different frequency (>100 Hz) of vibration from that of WBV. The combination of duration and sporadic nature of movement appears, with the markedly higher frequency, to cause the deleterious effects. In contrast, WBV employs low-amplitude (<10 mm) and low-frequency (<65 Hz) mechanical stimulation of the human body for short durations (<30 min) to attain an effective and safe way to exercise musculoskeletal structures.
History
In 1880, Jean-Martin Charcot, a French neurologist, examined the surprising improvements in the condition of pilgrims suffering from Parkinson’s disease. He surmised that such improvements were attributable to the vibration from the horse-drawn and railway carriages. Based on this idea he then developed a chair with a helmet that vibrated electrically. Between 1890 and 1910, Charcot’s ideas were developed further by different therapists. G. Taylor (USA), G. Zander (Sweden), and J. H. Kellogg (USA) produced different kinds of vibration therapy for the arms and back. In 1960, Dr. Biermann, a West German, published the paper ‘Influence of cycloid vibration massage on trunk flexion’ in the American Journal of Physical Medicine.
In 1970, Professor Vladimir Nasarov developed a vibration training programme as an effective method for athletes. He observed an improvement in power and flexibility using Biermann’s ideas in practical exercises. A short time later, this localized vibration training started to be used by the Russians in their space programme to prevent bone density changes in astronauts. They recognized that this new idea for exercise had the potential to provide suitable countermeasures for preventing bone and muscle loss for astronauts under microgravity conditions. WBV was later used to enhance the performance of Soviet athletes during their exercise training (Nasarov & Spivak 1985). These two authors were the first to highlight the association between strength and power development and whole-body or segment-focused vibration training. They assumed that repetitive eccentric vibration loads with small amplitudes would effectively enhance strength, because of a better synchronization of motor units.
Professor Nasarov was a Russian athletics coach who first applied vibration stimulation in sport. Basically, he wanted to help athletic performance based on the principle that by applying vibration to a distal muscle it would be transmitted to more proximal muscles. The special device he used generated vibration at a frequency of 23 Hz. Professor Nasarov found that the vibration produced an increase in the range of motion (ROM) of the involved joint, speculating that a shift in the pain threshold had occurred (Nasarov 1991 cited in Künnemeyer & Schmidtbleicher 1997). He also hypothesized that vibration training, besides improving flexibility, would also improve blood flow.
The first study (Fig. 1.1) which combined weight training and vibration training was performed by Issurin et al (1994). These researchers found a 46% improvement after weight training with vibration (3 weeks, three times a week, 44-Hz frequency with amplitude of 3 mm, 30 m/s2). The same weight training without vibration had a progression of only 16%.
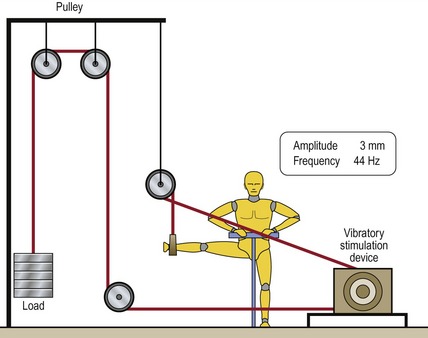
Figure 1.1 Combination of vibration training and weight training.
Reprinted from Issurin VB, Liebermann DG, Tenenbaum G (1994) Effect of vibratory stimulation training on maximal force and flexibility, Journal of Sports Sciences 12: 561–566, 1994, with permission from Taylor & Francis.
In a second study presented by Issurin and Tenenbaum (1999), 14 amateur and 14 elite athletes were subjected to vibratory stimulation during bilateral biceps curl exercises (Fig. 1.2) at a frequency of 44 Hz and with an oscillation of 3 mm peak to peak. They were also engaged in power exercises without vibration. The results in the elite athletes were an increase in explosive strength exertion for maximal and mean power of 10.4 and 10.2%, respectively, whereas in the amateurs the improvement was 7.9 to 10.7%.
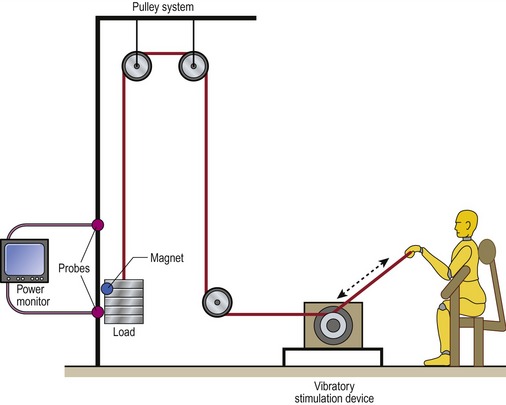
Figure 1.2 The bilateral biceps curl exercise and instrumentation.
Reprinted from Issurin VB, Tenenbaum G (1999) Acute and residual effects of vibratory stimulation on explosive strength in elite and amateur athletes. Journal of Sports Sciences 17: 177–182, with permission from Taylor & Francis.
In 1996, the first side-alternating vibration platform simulating the human gait was licensed in Germany. By 1998 vibration platforms with various types of displacement were available on the market. Those oscillating vertically have a different frequency from those oscillating side to side. Exercise programmes incorporating WBV have been tested in the areas of sports muscle strength, muscle power and muscle length (Bosco et al 1999a, Delecluse et al 2003, Issurin & Tenenbaum 1999); in gerontology, proprioception and balance training (Bautmans et al 2005, Bogaerts et al 2007, Runge et al 2000), bone density (Felsenberg 2004, Gusi et al 2006, Rittweger & Felsenberg 2004, Rubin et al 2002) and the rehabilitation of various musculoskeletal impairments associated with disuse atrophy, muscle spasms and low back pain (Belavý et al 2008, Fontana et al 2005, Rittweger et al 2002); and in people suffering from the effects of stroke (Tihanyi et al 2007, van Nes et al 2004) and Parkinson’s disease (Haas et al 2006).
Is vibration a natural stimulus?
During daily activity our body interacts with external forces. During walking and running our heel strikes the ground and absorbs this shock through pronation of the foot (McConnell 2002) and flexion of the knee (Perry 1992). These forces can also induce vibration and oscillations within the tissues of the body. Similarly, impacts related to sporting activity such as hitting the ball with a tennis racquet induce vibration. During, downhill mountain biking, vibrations are dissipated in the tissues through the arms. During downhill skiing, vibrations under the skis are captured by the body. Hence, through various structures such as soft tissues, bone, cartilage, synovial fluid, muscular activity and joint kinematics, the body not only dissipates the impact of the shocks, but also has a mechanism which regulates the transmission of these external forces (vibrations) into the tissue of the body (Cardinale & Wakeling 2005). It appears that the body is capable of tuning its muscle activity in order to reduce the vibrations that are passing through the soft tissue and which could have detrimental effects on it (Nigg 1997). Importantly, the amount of muscle activity required is related to the level of external vibration forces applied. A maximal activated muscle can dampen vibrations so that the oscillations within the tissues are diminished or eliminated (Wakeling et al 2002).
A ‘concept of tissue homeostasis, the envelope of function’, was proposed by Dye (1996), in order to explain anterior knee pain. This concept can be generalized to any musculoskeletal condition where the amount and frequency of loading is considered too large for the underlying structures. For example, while a weightlifter can normally lift over three times his body weight without any problems, a normal worker would not be able to do such a task and would probably become injured from such a huge effort. In such an instance, the normal worker would be outside his threshold, which could result in tissue breakdown (McConnell 2003). Dye (1996) described four factors pertinent to determining the size of the envelope of function: anatomical (involving morphology and biomechanical characteristics of tissue), kinematic (involving dynamic control of the joint), physiological (involving the mechanism of molecular and cellular homeostasis that determines the quality and rate of repair of the damaged tissues) and treatment (including the type of rehabilitation conducted by the therapist or the type of surgery that the patient has received).
Muscle can dampen external vibration and increase its activity in order to tolerate more vibration energy (Ettema & Huijing 1994). However, one must bear in mind that, according to Dye’s theory, the body needs a certain time to adjust to the load, and therefore probably to vibration.
Related posts:
 Theoretical considerations in the clinical application of WBV to sarcopenia, osteoporosis and metabolic syndrome
Biomechanics: Principles of WBV
Indications and contraindications in the clinical application of WBV: Immediate and long-term effects and their influence on the selection of dosage
Whole body vibration: Treatment with patients or athletes
WBV as a warm-up prior to sport: Effects on flexibility
Special Considerations for Type 1 and Type 2 Diabetes Mellitus
Theoretical considerations in the clinical application of WBV to sarcopenia, osteoporosis and metabolic syndrome
Biomechanics: Principles of WBV
Indications and contraindications in the clinical application of WBV: Immediate and long-term effects and their influence on the selection of dosage
Whole body vibration: Treatment with patients or athletes
WBV as a warm-up prior to sport: Effects on flexibility
Special Considerations for Type 1 and Type 2 Diabetes Mellitus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


