4 Indications and contraindications in the clinical application of WBV
Immediate and long-term effects and their influence on the selection of dosage
Indications
Whole body vibration (WBV) has been advocated for:
















Contraindications
WBV may be considered harmful in people with conditions such as:
Clinical research on acute and long-term effects of WBV
Vibration protocols can vary in the characteristic of the vibration (vertical vs rotational) as well as the frequency employed. Abercromby et al (2007a) in their study determined the effects of static and dynamic squatting, muscle contraction type using two types of vibration direction, rotational vibration (RV) and vertical vibration (VV) and removing large vibration-induced artefacts from EMG data which is what they also proposed as conclusion of the study. They found that the average responses of the extensors were significantly greater during RV than VV, whereas responses of the tibialis anterior were significantly greater during VV than RV. In their second study, Abercromby et al (2007b) evaluated quantitatively vibration exposure and biodynamic responses during typical WBVT regimens using two different types of vibration, as in the previous study, rotational vibration (RV) and vertical vibration (VV). The key finding of this study was that the risk of adverse health effects would be lower on a short duration exposures to RV (rotational vibration) than VV (vertical vibration) and at half-squats (small knee flexion angle 26-30°) rather than full-squats or upright stance. Furthermore, the parameter of amplitude also varies widely and frequently remains undefined. The duration of the exposure on the platform and the length of time between the cessation of the vibration exposure and the commencement of post-treatment measurements are other important factors which can modify the outcome of the clinical results. Additional variables include the position of the body during WBV, the degree of muscle contraction which can affect the biological response to vibration (Griffin 1997) and the specific movements tested following the vibration treatment.
As the populations using WBV vary markedly, so do the outcome measures. It has been reported that WBV may be an effective intervention for warming up for athletic events as well as for general exercise regimen (Cochrane et al 2007, Jordan et al 2005). Other investigations report significant improvements in disability and vitality measures in institutionalized elderly people (Bautmans et al 2005, Bruyere et al 2005, Kawanabe et al 2007, Roelants et al 2004a,b), while others have reported improvement in measures of strength in animals (Rubin et al 2007), blood flow (Stewart et al 2004) and bone mineral density (BMD) (Verschueren et al 2004) in post- and perimenopausal women. Additionally, neurological conditions such as Parkinson’s disease (Haas et al 2006), multiple sclerosis (Schuhfried et al 2005) and stroke (van Nes et al 2004) have also been treated with WBV. Hereby, it can be seen that the populations using WBV vary widely, which makes comparisons difficult. Nevertheless, what can be gleaned from these investigations is that a frequency of <20 Hz is used for muscle relaxation, whereas those between 26 and 44 Hz are used for improving issues related to muscle power and strength. Stimulation to the lower limbs above 50 Hz is thought to cause severe muscle damage (Rittweger et al 2002a). Duration generally does not exceed 10 min, in which the total initial stimulation is in the order of a few minutes with breaks between repetitions. Thus, the duration is progressive and incremental, depending upon the clinical outcomes being achieved.
Acute effects of WBV using the variables of duration, frequency, body positioning and amplitude
Most of the investigations to date have concentrated on the effect of WBV on functional neuromuscular performance in terms of muscle power and strength. In particular counter movement jump (CMJ), vertical jump, running speed and balance have been used as outcome measures. Other measures of the acute effects of WBV were taken using hormonal concentrations and cardiovascular changes. Moreover, the acute effects of WBV vary, depending upon the loading capacity and condition of the individual. Therefore, the dosage prescribed must be safe while still representing an efficacious loading for stimulating anabolic responses to the musculoskeletal system.
Amplitude and frequency
Rittweger et al (2002b) investigated the effect of frequency and demonstrated that vibration at an amplitude of 5 mm was accompanied by a linear increase in oxygen consumption from 18 to 34 Hz and that at 26 Hz the oxygen consumption increased more than proportionally with amplitudes from 2.5 to 7.5 mm.
Bruyere et al (2005) used peak-to-peak amplitudes of 3 and 7 mm with 10 and 26 Hz using a crossover design in institutionalized elderly. A vertically oscillating platform was used to determine the optimal WBV stimulus (frequency × amplitude), 2 and 4 mm at 25, 30, 35, 40 and 45 Hz. Unfortunately these authors did not report specifically on any variation in effect of these changes in parameters, and ideally the amplitude should have been changed without any changes in frequencies to really determine the effect. Nevertheless, it was found that higher WBV amplitude (4 mm) and frequencies (35, 40, 45 Hz) resulted in the greatest increases in electromyogram (EMG) activity (increase in vastus lateralis by 2.9–6.7% in static and 3.7–8.7% under dynamic conditions: Hazell et al 2007).
Body positioning and fatigue
Body positioning and its acute effects is another parameter which can define the prescription of dose. A person standing on a platform requires muscle activation from the lower limbs in order to dampen the vibrations coming up from the vibrating plate (Rubin et al 2003, Wakeling et al 2002). Using intramedullary pins in the greater trochanter and L4 vertebra, researchers were able to demonstrate decreased transmissibility of vibration with varying postures. In relaxed stance transmissibility reduced to 30%, with 20° knee flexion transmissibility reduced to 30%. Additionally, a phase-lag, as high as 70°, occurred between the hips and lumbar spine (Rubin et al 2003). In this study, a unique vibration platform developed for use in a clinical setting was used to impose the WBV. The platform was driven to provide a force of 36Np_p at all loading frequencies, with data collection recorded at 2 Hz, intervals at 15 Hz and finishing at 35 Hz. Rittweger et al (2001) measured an increase in the rate of oxygen consumption during the exposure to vibration. During this research, these investigators not only utilized WBV training but also added dynamic changes in body position in addition to extra loads of up to 40% of the subject’s body weight at their waists until exhaustion. Rittweger et al (2001) tested 37 young healthy subjects standing with their feet 15 cm away from the axis of rotation on either side of a platform with a horizontal displacement. Vibration frequency of 26 Hz and a peak acceleration force of 15g were used. The authors compared two WBV exercise sessions with bicycle ergometry. Heart rate, blood pressure and oxygen uptake and perceived exertion on Borg’s scale increased. Systolic arterial blood pressure and heart rate were found to have increased after WBV but less so than after bicycle ergometry. In contrast, diastolic blood pressure had decreased only after WBV. However, after WBV, jump height was reduced by 9.1%, voluntary force in knee extension reduced by 9.2% and the reduced muscle electromyography (mEMG) during maximal voluntary contraction was attenuated. Taking these results together, one can hypothesize that there are probably two mechanisms of fatigue a neural one and a muscular one. Furthermore, this demonstrates that WBV elicits a metabolic muscular response and therefore is not a passive form of exercise. Oxygen consumption is increased 4.5 mL/min/kg Rittweger et al (2001); this is comparable to walking at 0.4 m/s, which requires 2.3 mL/min/kg.
Muscle function
Torvinen et al (2002a), using a randomized crossover design, tested 16 young adults to investigate a 4-min vibration bout on muscle performance and body balance. A tilting plate, Galileo, was utilized for the intervention where the subjects were asked to stand in different manners. These included a relaxed position, light squatting, on the heels, light jumping and alternating the body weight from one leg to another. The vibration frequency increased in 1-min intervals from 15 Hz by the first minute to 30 Hz for the last minute. The test was performed on 2 days, WBV versus non-WBV, or sham-loading. The peak-to-peak amplitude was 10 mm, with a maximal acceleration of 3.5g (where g is the Earth’s gravitational field or 9.81 m/s2). Six performance tests were conducted 10 min before (baseline), and 2 and 60 min after the intervention. Bipolar surface EMG from soleus, gastrocnemius and vastus lateralis muscles were recorded during the 4-min bout of WBV intervention. The vibration loading, based on the Galileo tilting plate, induced a transient increase (especially on the 2-min test) in the isometric extension strength of the lower extremities by 3.2% (p = 0.020), a 2.5% (p = 0.019) benefit in the jump height and a 15.7% improvement in the body balance (p = 0.049). Interestingly, these effects were seen at 2 min, but had disappeared more or less completely after 1 hour. A decrease EMG mean power frequency (mpf) of all muscles during the vibration was seen, indicating that a long-term irritation of the muscle-spindle by vibration leads to muscle fatigue (Eklund 1972).
In another study, Issurin and Tenenbaum (1999) examined 14 elite and 14 amateur athletes who were subjected to vibratory stimulation during bilateral biceps curl exercises using explosive strength exertion. Each subject performed two separate series of three sets of bilateral biceps curls in random order. In the second set of one series, a vibration stimulus was administered through a cable to the handle and therefore to the arm muscle. The stimulus frequency was 44 Hz with an amplitude of 3 mm. Elite and amateur athletes showed an improvement of 10.4 and 7.9%, respectively, in maximal power attributed to vibratory stimulation. In contrast, 65-Hz stimulation directly to the biceps tendon reduced neuromuscular performance (Moran et al 2007). Hence, frequencies of <50 Hz are used.
Hormones and muscle function
Carmelo Bosco, Marco Cardinale and colleagues conducted several investigations over the past several years whereby they reported that WBV interventions would enhance strength and power in well-trained people. Besides the improvements in muscular power, in his PhD thesis, Cardinale (2002) also demonstrated that WBV produces an immediate effect on hormone levels. These results included increased testosterone by 7%, increased growth hormone by 460% and reduced cortisol by 32%. The last finding suggests that WBV is not a stressful experience in physically active individuals, when the 10-min protocol was subdivided into two sets of five subsets, lasting 1 min each with a 6-min rest between sets. However, when a protocol of 7 min of constant WBV was used, vertical jumping ability actually declined and cortisol concentrations actually rose. Therefore, precise dosage in terms of sets and rest periods are important.
Bosco et al (1999a) evaluated the influence of vibration on the mechanical properties of arm flexors, in a group of 12 international-level boxers. The experiment consisted of five repetitions lasting 1 min each with mechanical vibration (30 Hz, 6-mm displacement). The results showed an increase in power output by 12% in unilateral bicep curl. Investigating the lower extremity, Bosco et al (1999b) demonstrated that 10 min (10 times 60 s) of whole body vibration training (WBVT) at 26 Hz with 10-mm peak-to-peak amplitude, on well-trained volleyball players, improved vertical jumping ability. In a follow-up investigation, in young men, they demonstrated increased concentrations of testosterone and growth hormone and also decreases in the blood concentration of the body’s stress hormone, cortisol (Bosco et al 2000).
These astonishing results on hormones have been used, and abused, by various companies to promote WBVT and exercises as well as to sell WBV platforms, as ‘it boosts hormones, like testosterone and growth hormone, and reduces cortisol and stress whilst enhancing muscle remodelling.’ One should not lose sight of the fact that there are also numerous studies which do not show any improvement in strength/power performance and hormone concentrations. Additionally, several limitations of these studies include small numbers (n = 6, 12 and 14), with the latter not randomly assigned and therefore without a control group. Bosco et al (1999a,b) also did not indicate in either study the duration between the WBVT and the measurements of their effect, which is essential information for the reproducibility of these results in future trials.
Two investigations, by De Ruiter et al (2003a) and Di Loreto et al (2004), demonstrated no improvement with WBVT. In the work of De Ruiter et al (2003a), subjects exercised on a vibration platform using five sets of 1 min with a frequency of 30 Hz and amplitude of 8 mm, but with 2 min rest between sets. The result showed a reduction in maximal voluntary knee extension force. Of note is the difference in the protocol, in which the 2-min rest period between sets is quite different from other studies. Di Loreto et al (2004) did not notice any change in serum concentrations of growth hormone insulin-like growth factor 1 (IGF-1) and free and total testosterone. In their investigation, WBVT was performed for 10 min at 30 Hz albeit using relatively small amplitude. Since no change in serum levels of IGF-1 could be seen, investigations of intramuscular IGF-1 may be more beneficial in determining a muscular growth-stimulating effect. On a positive note, Di Loreto et al (2004) did find that vibration slightly reduced plasma glucose (30 min: vibration 4.59 ± 0.21, control 4.74 ± 0.22 nM, p = 0.049) and increased plasma norepinephrine concentrations (60 min: vibration 1.29 ± 0.18, control 1.01 ± 0.07 nM, p = 0.038).
Swelling and erythema
Swelling and erythema of the foot after WBV, particularly in the first session and especially in women, was observed by Rittweger et al (2000). Also itching was reported frequently, but these changes resolved rapidly if the subjects walked around. The question that arises is whether the swelling and erythema are caused by vasodilation of supplying arteries via an increase in perfusion pressure or whether it is a direct mechanical effect. Since the oedema and erythema were observed on the plantar surfaces of the feet, i.e. the body part closest to the vibrating platform, Rittweger et al (2000) concluded that the explanation was a direct mechanical one.
Blood flow
Another study examined alterations in muscle blood volume (Kerschan-Schindl et al 2001) with power Doppler sonography of the arterial blood flow of the popliteal artery. Twenty healthy adults stood with both feet on a tilting platform in three different positions for 3 min each without breaks in between. The amplitude was 3 mm and the frequency 26 Hz. The result of the study demonstrated an increase in mean blood flow velocity in the popliteal artery from 6.5 to 13.0 cm/s. Other investigators have demonstrated enhanced peripheral and systemic blood flow (25–35%), with improved lymphatic flow and better venous drainage (Stewart et al 2004). This suggests that low-frequency vibration does not have the same negative effects on peripheral circulation as seen in occupations with exposure to prolonged low-frequency vibration.
Proprioception and low back pain
In a pilot study by Fontana et al (2005) the effect of weight-bearing exercise in conjunction with low-frequency WBV was investigated to determine whether this combination would improve lumbosacral position sense in healthy subjects. Since patients with low back pain (LBP) often present with impaired proprioception of the lumbopelvic region (motor control dysfunction), which contributes to neuromuscular dysfunction and thereby impaired segmental stability (O’Sullivan et al 2003), the use of WBV may provide a useful treatment tool. Twenty-five individuals (eight men and 17 women) between the ages of 19 and 21 were randomly assigned to the experimental group (n = 14) and to the control group (n = 11). The experimental group received WBV using Galileo for 5 min with a frequency of 18 Hz and an amplitude of 10 mm (feet were placed apart). For the entire time the participants had to maintain a static semi-squat position during the WBV. The control group adopted the same position for an equal time but without receiving any vibration. A two-dimensional motion analysis system measured the repositioning accuracy of the pelvic tilt in standing was used. The results demonstrated that 5 min of WBV induced a decrease in absolute mean repositioning error, improving repositioning accuracy by 39% or 0.78°. Moreover, this was not dependent on the anterior or posterior repositioning of the pelvis. The net proportional benefit of the experimental group over the control group after the test was 53%. It was therefore concluded that WBVT has an effect on lumbosacral proprioception which had not been assessed in previous studies. Furthermore, this effect occurred with such a small amount of WBVT. These authors also stated that these results could provide a possible explanation for the beneficial findings by Rittweger et al (2002a) in their 12-week treatment programme in which they found an improvement in function and a relief in pain in patients with LBP. Further explanations for improved proprioception were also provided by Belavý et al (2008), who found that 8 weeks of WBV stimulated lumbar multifidus function. Atrophy of the multifidus muscle and loss of its proprioceptive function has been shown to be a significant contributor to chronic LBP (Hides 1996, Hodges 2004). Finally, Di Loreto et al (2004) found that WBV increased plasma norepinephrine concentrations (60 min: vibration 1.29 ± 0.18, control 1.01 ± 0.07 nM, p = 0.038). Direct descending noradrenergic pathways in the spinal cord have profound forward modulating effects on pain; however, the blood–brain barrier precludes plasma norepinephrine passing into the spinal cord. An indirect pathway for the resolution of pain may occur through the immune-inflammatory response as peripheral noradrenergic receptors innervate the blood vessels of the spleen, bones, nerves and lymphatic system.
Parkinson’s disease
Vibration training has also been used to improve the symptoms of Parkinson’s disease. Haas and colleagues (2006) have shown that 68 patients (15 women and 53 men) using WBVT have experienced improvements in one or more symptoms. A crossover design was used to control treatment effects on motor symptoms, which were assessed by the Unified Parkinson’s Disease Rating Scale (UPDRS) motor score (Fig. 4.1). The treatment consisted of five sets of WBV lasting 60 s each with a 1-min pause between each series. The mean frequency of the vibration adopted was 6 Hz and the amplitude was 3 mm. In the treatment group, an improvement of 16.8% in the UPDRS motor score was found. The highest improvements were found in tremor and rigidity, 25 and 24%, respectively. Gait and posture showed an improvement of 15%, and bradykinesia scores were reduced by 12 on average, but no changes were found in cranial symptoms. It is worth emphasizing that these improvements were seen immediately after the intervention and lasted for 120 min, when the UPDRS score still had not returned to baseline. Moreover, correlation of the UPDRS with other functional psychometric questionaires and functional tests suggest that this is the strongest evidence yet for a (CNS) role in low-frequency WBV (Table 4.1).
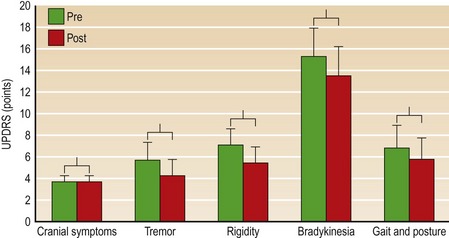
Figure 4.1 UPDRS motor scores before and after treatment in a five-symptom cluster.
Reprinted from Haas CT, Turbanski S, Kessler K et al (2006) The effects of random whole-body-vibration on motor symptoms in Parkinson’s disease. Neurological Rehabilitation 21:29–36, with permission
Related posts:
 Introduction
Theoretical considerations in the clinical application of WBV to sarcopenia, osteoporosis and metabolic syndrome
Biomechanics: Principles of WBV
Whole body vibration: Treatment with patients or athletes
WBV as a warm-up prior to sport: Effects on flexibility
Special Considerations for Type 1 and Type 2 Diabetes Mellitus
Introduction
Theoretical considerations in the clinical application of WBV to sarcopenia, osteoporosis and metabolic syndrome
Biomechanics: Principles of WBV
Whole body vibration: Treatment with patients or athletes
WBV as a warm-up prior to sport: Effects on flexibility
Special Considerations for Type 1 and Type 2 Diabetes Mellitus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


