Intertrochanteric Fractures
Andrew H. Schmidt and Richard F. Kyle
Key Points
• The treatment of intertrochanteric femur fractures is nearly always operative.
• Historically, cephalomedullary nails have been associated with higher rates of revision surgery than compression hip screws, largely because of the increased risk of postoperative femur fracture. However, this complication seems to be decreasing with current nail designs, and more recent series have found no increased risk of femoral fracture in patients treated with cephalomedullary nails compared with compression hip screws.1
Introduction
Intertrochanteric fractures of the upper femur occur in the region of the femur bounded by the femoral neck and lesser trochanter medially and the greater trochanter laterally. These fractures occur in two circumstances: with high-energy trauma in the younger patient, and following a simple fall in the older patient. The latter type of fracture is typically associated with senile osteoporosis. Intertrochanteric fractures present in a wide variety of patterns that range from simple to complex and may be minimally displaced or widely displaced. Similar to the proximal humerus, the proximal femur often fractures into typical fragments, which in the femur include the femoral neck and head, the greater and lesser trochanters, and the femoral shaft (Fig. 45-1). Extension of the fracture may occur distally along the femoral shaft, confusing the distinction between intertrochanteric fractures and subtrochanteric fractures.
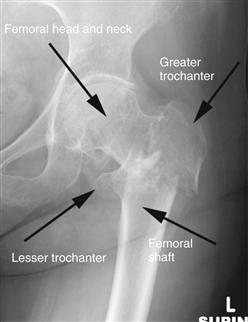
Figure 45-1 Anteroposterior radiograph of a comminuted intertrochanteric fracture, demonstrating classic fracture fragments and displacement. This particular fracture is an example of the newly described Kyle type V fracture, in which an associated fracture occurs at the base of the femoral neck.
These fractures are easily diagnosed in the patient with a known or suspected fall on the basis of pain and deformity of the limb, which typically is shortened and externally rotated. Plain radiographs confirm the diagnosis in most cases. Occasionally, a patient with hip pain has normal radiographs; in this case, magnetic resonance imaging should be done. Bone marrow edema or a cortical break in the trochanteric region can be considered evidence of a nondisplaced fracture.
The standard of care for these injuries is surgical stabilization. Nonoperative care of displaced fractures almost always results in varus malunion of the proximal femur with limb shortening and rotational deformity, unless some sort of skeletal traction can be maintained. Even more important, nonoperative care of displaced and/or unstable fractures requires prolonged recumbency of the patient, whereas patients usually can be mobilized in some manner immediately after surgery.
Indications/Contraindications
Nonoperative Care
Nonoperative treatment of intertrochanteric fractures is appropriate for those patients with radiographically occult fractures who can be mobilized without too much pain. If this approach is chosen, patients (and their families) need to be warned about the possibility of later displacement, and frequent radiographic follow-up is necessary. Rarely, patients with displaced fractures are not viewed as candidates for surgery or anesthesia because of severe medical comorbidities. When nonoperative management is chosen, such patients need careful medical management and attentive nursing care to prevent thromboembolism, malnutrition, decubitus ulcers, or other complications of prolonged recumbency. Large series reported in the literature indicate that results comparable with those reported after surgery can be obtained with skeletal traction.2
Operative Management
Historical Background
Intertrochanteric femur fractures have been managed traditionally with compression (also referred to as sliding) hip screws that allow collapse of the facture along the axis of the lag screw, thereby creating bone-to-bone contact that in turn increases stability and leads to reliable healing. The widespread adoption of the compression hip screw that occurred during the 1980s dramatically reduced the incidence of nonunion and loss of fixation that occurred with earlier fixed-angle devices. In the 1990s, cephalomedullary nails were introduced for use in intertrochanteric fractures, yet their role in the management of these fractures is still somewhat controversial. Intramedullary devices offer a potentially less invasive approach to fixation of intertrochanteric fractures compared with plate fixation with a compression hip screw. Recent investigations of the functional outcomes of elderly patients with unstable fracture patterns have highlighted problems associated with loss of reduction due to collapse, which in turn causes limb shortening and loss of the abductor moment arm with potential pain, limp, and poor functional outcomes (Fig. 45-2).3–5 Fracture collapse after initial reduction and fixation is less common when intramedullary devices are used, so that cephalomedullary nails are now commonly used in patients with unstable fracture patterns, such as those with loss of integrity of the lateral wall of the greater trochanter and reverse-obliquity fractures.5,6 However, large series of patients comparing compression hip screws with intramedullary nails demonstrate that patients treated with intramedullary nails have a higher overall rate of revision surgery during the first year.7 For these reasons, the compression hip screw remains the implant of choice at many centers for the treatment of intertrochanteric fractures.8

Figure 45-2 Serial anteroposterior radiographs of a patient showing progressive collapse of a compression hip screw comparing the immediate postoperative image (middle panel) with another image 5 months later (right panel). The arrow in the middle panel shows loss of integrity of the lateral wall of the greater trochanter, which is associated with excessive collapse when sliding hip screws are used.
Current Surgical Practice
Surgery is the standard of care for intertrochanteric fractures. Surgical options include external fixation, internal fixation with a compression hip screw, and internal fixation with an intramedullary device, typically a so-called cephalomedullary nail (sometimes referred to as an intramedullary hip screw). Any of these options can be considered for almost any fracture, and the optimum implant for a given fracture type is a matter of considerable debate.
External fixation is not commonly done, despite reports of success.9 Very few orthopedic surgeons have experience in the management of intertrochanteric fractures with external fixation, and the need for prolonged care of external fixation pins, as well as complications of pin infection and later fracture through pin sites, makes this technique unpopular.
Compression hip screws represent the traditional standard for operative care of intertrochanteric femur fractures. Loss of fixation is rare when the lag screw is placed within the center of the femoral head, as noted by Kyle and associates10 and more recently quantified by Baumgaertner and colleagues11 as the so-called tip-apex distance (TAD). Although compression hip screws can be used successfully with any fracture of the proximal femur,8 recent evidence suggests that use of these devices in specific unstable fracture patterns may lead to increased collapse and/or loss of fixation. Traditionally, loss of the posteromedial buttress of the proximal femur, including the posterior aspect of the femoral neck and the lesser trochanter, has been considered the hallmark of instability (Fig. 45-3). Kyle and coworkers documented that collapse, cutout, and nonunion occurred in 25% of patients with a combined intertrochanteric-femoral neck fracture, which they newly described in their paper.3 This particular type of fracture, which they described as the Kyle type V fracture, has severe comminution of the greater trochanter and associated femoral neck fracture (see Fig. 45-1), which led to complete collapse of the sliding hip screw in nearly half of the cases in their series, and in 100% of failed cases.3 Other authors have highlighted loss of the integrity of the lateral wall of the greater trochanter as a risk factor for loss of reduction with compression hip screws (see Fig. 45-2, middle panel).6,12,13 Another fracture pattern that is widely considered to be a contraindication for the use of a compression hip screw is the reverse-oblique fracture (Fig. 45-4). The general consensus, supported by the literature, is that use of a compression hip screw in reverse-oblique fractures leads to frequent complications (Fig. 45-5).14,15 These unstable fracture patterns must be recognized because recent literature has documented shortening of the femoral neck, loss of the abductor moment arm, limb length discrepancy, and, most important, poorer functional outcomes in patients with unstable fractures treated with compression hip screws.16,17 Thus, routine use of compression hip screws in unstable fracture patterns, such as those with loss of the lateral buttress, is now discouraged.

Figure 45-3 Example of an intertrochanteric femur fracture with a large posteromedial fragment (arrow).

Figure 45-4 Preoperative (left panel) and postoperative (right panel) anteroposterior radiographs of a reverse-obliquity fracture of the proximal femur, reduced and stabilized with a cephalomedullary nail.

Figure 45-5 Example of catastrophic loss of fixation of a reverse-obliquity fracture treated with a sliding hip screw. Note the evidence of toggling of the lag screw within the femoral head, which occurred after the sliding screw collapsed maximally, and before ultimate failure by pulling out of the screws from the femoral shaft.
Intramedullary implants, such as the cephalomedullary nail, are being used increasingly for intertrochanteric fractures (Fig. 45-6). Cephalomedullary nails are available in both short and long versions. Short intramedullary devices have been plagued by intraoperative and postoperative fractures.17–24 In contrast, long cephalomedullary nails have been associated with anterior femoral cortical perforation due to mismatch between the radius of curvature of these nails and the femur.25,26 This is more of an issue when most of the femoral canal is intact, as is the case when nails are used for very proximal femoral fractures.26 Intramedullary nails have theoretical benefits. First, their intramedullary position buttresses the proximal femur, thereby preventing excessive collapse of the femoral neck and preventing shortening. Second, by virtue of the more medial position, they experience less loading because of a shorter moment arm. However, as was pointed out by Zlowodzki and associates, this is true only for 135-degree compression hip screws; a high-angle (150-degree) hip screw actually has a shorter moment arm than a 135-degree intramedullary hip screw.27 In addition, neck shaft angles of intramedullary nails are usually limited to a few angles (typically 125 or 130 degrees) that are “built in,” and the position of the guide pin is determined by the position of the nail in the femur, so that achieving ideal center-center position of the lag screw within the femoral head is potentially more difficult to attain with these devices.28 This is especially true in patients with a neck shaft angle less than 125 degrees, in whom a sliding hip screw would allow better implant placement within the femoral head.28

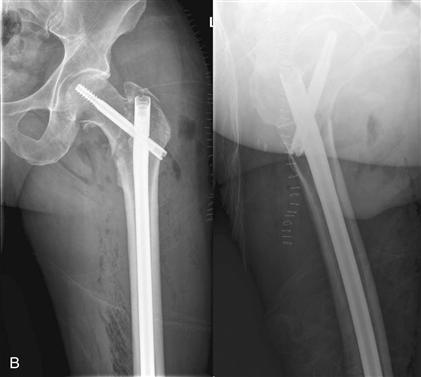
Figure 45-6 Example of an intertrochanteric fracture of the femur treated with a cephalomedullary nail. A, Preoperative anteroposterior and lateral radiographs. B, Postoperative radiographs following reduction and cephalomedullary nailing.
Another important difference between compression hip screws and cephalomedullary nails is their relative cost. Nails may cost three to four times more than a standard compression hip screw. This fact must be considered in light of evidence that overall outcomes remain good in patients treated with the less expensive compression hip screws,8 and that overall revision surgery rates at 1 year may be higher in patients treated with nails.7
Evidence-Based Approach to Choice of Fixation
The decision regarding choice of a compression hip screw or a cephalomedullary nail for a given patient is complex and depends on many factors related to the patient, the fracture, the surgeon, and the environment in which care is provided. Therefore, it is worthwhile to develop an evidence-based approach to the care of these injuries.
A number of level I and II prospective clinical trials have been published that compare compression hip screws with intramedullary devices.* Although a detailed analysis of all of these studies is beyond the scope of this chapter, they can be summarized as follows (Table 45-1). In general, no consistent, statistically significant, and clinically relevant differences have been found among any perioperative factors between groups of patients treated with a compression hip screw or a cephalomedullary nail. In contrast, functional differences, when present, seem to be of a larger magnitude and favor intramedullary devices, especially in unstable fracture patterns.4,5,16,17,24 Finally, distinct differences in complications are evident, with femoral shaft fracture complicating many reported series of cephalomedullary nails,18,19,24,29 whereas loss of reduction and implant cut-out are more common following use of a compression hip screw, especially in unstable fractures characterized by loss of integrity of the lateral wall of the greater trochanter, associated femoral neck fracture, or extension in the subtrochanteric region of the femur.3,6,12,13,18
Table 45-1
Summary of Level I and II Studies Comparing Intramedullary Fixation Versus Compression Hip Screws for Intertrochanteric Fractures
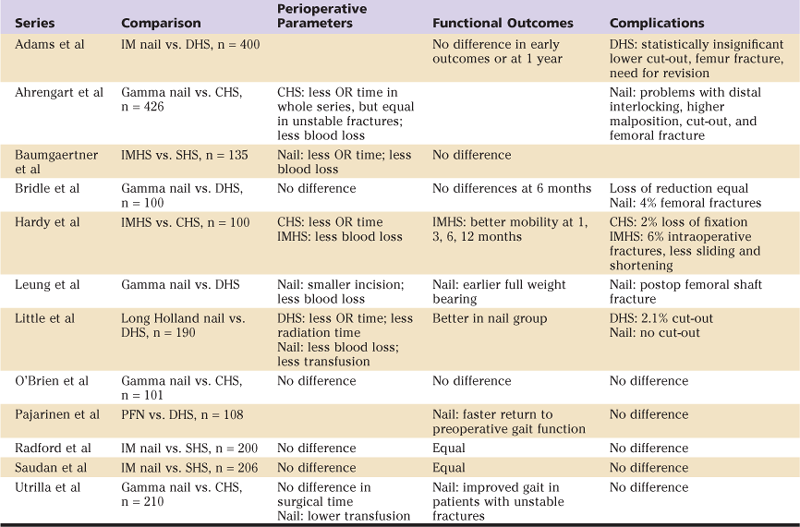
CHS, Compression hip screw; DHS, dynamic hip screw; IM, intramedullary; IMHS, intramedullary hip screw; OR, operating room; PFN, proximal femoral nail; SHS, sliding hip screw.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


