CHAPTER 69 Interposition Arthroplasty of the Elbow
HISTORICAL ASPECTS
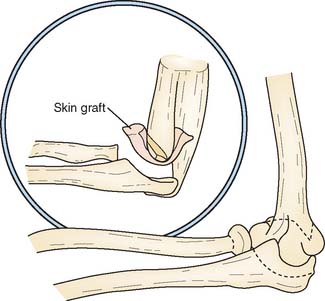
The so-called functional arthroplasty, popularized by Hass (1944),11 might be considered the predecessor of interposition arthroplasty. Functional arthroplasty is actually a variation of resection arthroplasty, except that the distal humerus is fashioned in the shape of a wedge and various types of interposed tissues may be inserted (Fig. 69-1). Hass reported a long-term satisfactory result of 73% in 15 patients, with an average follow-up period of 5.5 years. Because this is a type of resection arthroplasty, it is not surprising that 13 of the 15 procedures were in patients with previous infection.
Interposition arthroplasty has been used for treatment of arthritis involving the temporomandibular, shoulder, wrist, knee, and hip joints. Of these, the elbow has been reported as second only to the temporomandibular as the joint most amenable to the technique.13 In Europe, arthroplasty was popularized by Putti30 and by Payr.28 Schüller was the first to recommend the procedure for patients with rheumatoid arthritis.32 Various muscle flaps, pig bladder,2 fascia-fat transplants, skin, and other materials have been used as the interposing agent. In 1902, Murphy introduced and popularized arthroplasty in the United States.26,27 Lexer,21 in 1909, emphasized the value of autogenous tissue and confirmed the impression of Murphy27 that fat and fascia were the best substances for interposition arthroplasty. He reported that fascia remained viable and was replaced by fibrous and fibrocartilaginous tissue. The observation has not been subsequently confirmed, rather the joint appears to be comprised primarily of fibrous tissue.29
OUTCOMES
Autogenous or xenograft cutis has been used as an interposing membrane in resection arthroplasties (cutis arthroplasty) of various joints since 1913, and successful use in the elbow has been reported by several authors.9,16,24 Cutis is the thick dermal layer of skin that remains after the superficial epidermal layer has been removed. It is a tough, durable, elastic membrane, and it closely adheres to the cut surface of the distal humerus.
Fascia lata is easy to harvest and conforms readily to the bony surfaces, but the donor site leaves variable morbidity. Efforts to enhance its effect have been reported by Kita17 using chromicized fascia lata, the so-called J-K membrane.
In 1979, Shahriaree and colleagues33 reported that of 30 patients, 90% returned to their previous occupations after excisional arthroplasty with Gelfoam interposition. Smith and associates34 successfully used silicone sheets as interposition material in six patients with hemophilic arthropathy.
INDICATIONS
INTERPOSITION
Specific Indications
The basic indications for interposition arthroplasty are either incapacitating pain or loss of motion in an individual younger than 40 years of age with rheumatoid arthritis, and younger than 60 years of age with traumatic arthritis. Loss of motion may follow trauma, sepsis, burns, or degenerative or inflammatory arthritis. However, the most compelling indication for arthroplasty of the elbow is incapacitating functional loss. If the loss of motion and pain are postinfectious, careful evaluation must be done to ensure that the patient has been free of the infection, preferably for at least 1 year. The best indication for this procedure is post-traumatic, painful loss of motion not complicated by sepsis in an individual who does not require long-term heavy demand on the joint.25
CONTRAINDICATIONS
If recent sepsis has occurred, other than débridement, reconstruction should not be considered. If epiphyseal closure has not occurred, arthroplasty should be delayed until growth is complete. In the past, a major contradiction to interposition arthroplasty was inadequate bone stock. Grishin and colleagues,10 however, have reported using interposition arthroplasty in conjunction with reconstructive bone grafts for marked osseous deficiency.
We have found gross instability, deformity, and marked pain, especially at rest, are all associated with poorer outcomes.8,20,25 The patient with a grossly unstable elbow from rheumatoid or post-traumatic arthritis cannot be adequately stabilized by an interposition procedure. Congenital ankylosis of the elbow joint that lacks the necessary ligamentous support may be treated with interposition and ligamentous reconstruction. However, the absence of flexion motor power is an absolute contraindication to this procedure. The need to use the upper extremity in ambulation or for transfer from bed to chair is a relative contraindication because excessive loading of the elbow destabilizes the joint.
PREFERRED TISSUE
Autogenous skin and fascia and achilles tendon allografts have all been used by the senior author. The cutis is very durable and thick, rapidly adheres to the bone, and has generally been successful.4,7,9 The harvest techniques are attractive in those patients in whom primary closure may be carried out. Cutis tissue without the epidermis is somewhat more difficult to harvest. Fascia is also commonly used because it is readily available from the thigh and can be overlapped to ensure adequate bulk.18,25 Recently other processed tissues such as AlloDerm (LifeCell, Branchburg, NJ) are being investigated for this purpose.12 At present, we prefer the achilles tendon allograft because it is readily available. The following anatomic features are required for success of the procedure: absence of donor site morbidity, large size and thickness, sufficient material for ligament reconstruction if necessary, and presence of calcaneus if osseous graft is required.
PREFERRED TECHNIQUE—ACHILLES TENDON ALLOGRAFT
SURGICAL TECHNIQUE
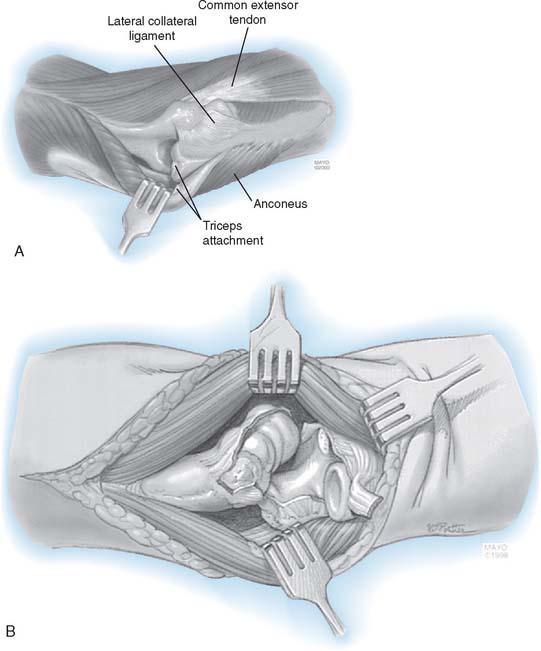
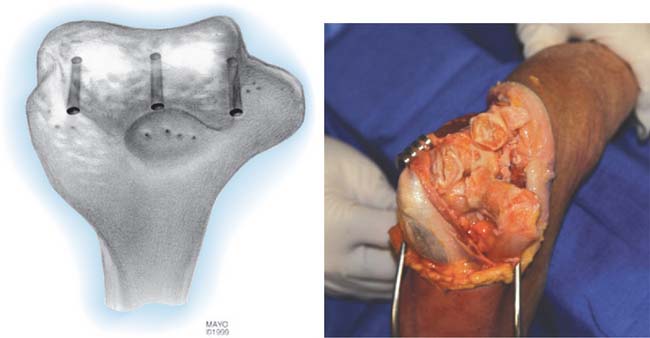
The patient is positioned supine with a pneumatic tourniquet in place. A posterior incision is preferred, although a pre-existing incision is reopened if consistent with the needed deep exposure. In all instances, the ulnar nerve is identified, mobilized, and protected throughout the case. The nerve is transposed subcutaneously if it is found to subluxate at the completion of the surgery. Kocher’s interval is developed between the anconeus and extensor carpi ulnaris. The lateral collateral ligament (LCL) complex and the common extensor muscles are released from the lateral condyle of the humerus. Anterior and posterior capsulectomy is performed to obtain useful elbow motion (Fig. 69-2). The tip of the olecranon is removed if it is prominent. The triceps muscle is elevated from the lateral distal humerus, and the anconeus mobilized from its ulnar attachment. The lateral one half of the triceps attachment is released from the olecranon, and the extensor mechanism is inserted as the forearm is flexed and supinated. If the cartilage appears beyond salvage, then the decision is made to proceed with interposition arthroplasty. The ulnar and humeral surfaces are prepared with a rongeur, burr, or semicircular saw to obtain a congruent articulation (Fig. 69-3). Care is taken to avoid resection of the subchondral bone, which may lead to excessive bony resorption, although the medial and lateral trochlear ridges are removed if necessary to obtain a smooth articulation. Sufficient bone is resected from the ulnar and humeral articular surfaces to accommodate at least 2 to 3 mm of joint space laxity even after insertion of the tendon to avoid “overstuffing” the joint.
Graft Application and Ligament Reconstruction
A fresh-frozen Achilles tendon allograft is our current preference (Fig. 69-4). Three or four drill holes are made across the distal humerus (see Fig. 69-3). Using a horizontal mattress stitch, the graft is sutured to the distal humerus through the drill holes (Fig. 69-5). The ulnohumeral joint is then reduced, and the integrity of the medial collateral ligament (MCL) is assessed. The smoothness of the articulation and elbow range of motion are determined. If adequate tissue is present, the lateral collateral ligament is repaired primarily. If the tissue is inadequate, reconstruction of the remaining portion of the ligament is carried out with the allograft tendon (Fig. 69-6). In cases in which both lateral and medial collateral ligaments are intraoperatively found to be deficient, a tunnel is drilled through the distal humerus, replicating the axis of rotation at the ulna. A second tunnel connects the sublime tubercle and the tubercle of the crista supinatorus. The distal strands of the allograft are threaded through the humeral tunnel and ulnar tunnels to create a “sling” simultaneously to reconstruct both the MCL and LCL (Fig. 69-7). The sling is hand-tensioned to maintain joint stability but still allow for smooth flexion and extension across the articulation. Following the reconstruction, the elbow is again taken through a range of articulated motion and tested for stability.







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


