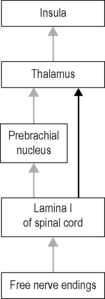
2.3 Interoception Disorders such as anxiety, depression, or irritable bowel syndrome have subsequently been described as interoceptive disorders. Most notably, it has been proposed that the neural pathways associated with interoception may be considered as a potential correlate for consciousness (Craig 2009). The sensory receptors for interoception are free nerve endings, most of which are located in fascial tissues throughout the human body. It is helpful to understand that proprioception and interoception are organized differently in the human brain and that very different afferent pathways are involved in them. Previous concepts of interoception often focused on visceral sensations only. Current concepts describe interoception as a sense of the physiological condition of the body, which includes a much wider range of physiological sensations, including, for example, muscular effort, tickling, or vasomotor sensations (see Box 2.3.1). These sensations are triggered by stimulation of unmyelinated sensory nerve endings (free nerve endings) that project to the insular cortex rather than to the primary somatosensory cortex which is usually considered as the main target of proprioceptive sensations (Berlucchi & Aglioti 2010). A recent and surprising addition to the above list of interoceptive sensations is the sense of sensual or pleasant touch. This discovery was triggered by examinations of a unique patient lacking myelinated afferents in whom slow stroking of the skin with a soft brush triggered a faint and obscure sensation of pleasant touch (and general well-being), although the patient was unable to recognize any stroking direction. Functional magnetic imaging showed that this vague sensation was accompanied by a clear activation of the insular cortex, while no activation was seen in the primary somatosensory cortex. (Olausson et al. 2010). Based on the innervation of primate skin and on subsequent studies with other patients it was concluded that the affected sensory receptors are unmyelinated C-fiber afferents with a low mechanical threshold, and that these endings are themselves connected with neural interoceptive pathways. Those afferents have a slow conduction velocity (0.5–1.0 s delay from stimulus to arrival in the brain). Since these receptor types have never been found in the palm of the hand despite numerous microneurographic recordings, it is assumed that they are present in hairy skin only and are absent in glabrous skin. It is concluded that human skin contains particular touch receptors which form a system for social touch that may underlie emotional, hormonal (for example oxytocin), and affiliative responses to caress-like, skin-to-skin contact between individuals (Fig. 2.3.1). The profound importance of such a system for human health and well-being has long been indicated (Montague 1971), at least since the classical study of Harlow (1958) with baby rhesus monkeys that express affection for a surrogate mother in response to tactile comfort. Interestingly, this particular “lamina I spinothalamocortical pathway” is a comparatively recent phylogenetic acquisition of primates. It evolved from the afferent portion of the evolutionary ancient system that maintains the homeostatic integrity of the body. In mammals, the activity of lamina I neurons is integrated in the parabrachial nucleus; it is only from there that they are further projected to the insular cortex via the ventromedial thalamic nucleus (Craig 2009). In primates, however, there are direct projections from lamina I to thalamic regions from which they are further conveyed to the insular cortex (Fig. 2.3.2). In other words, primates possess a more direct route between the afferent region for interoceptive sensations in the spinal cord (lamina I) and their insular cortex. No comparable difference in terms of neuronal architecture between primates and other mammals has been observed regarding their processing of proprioception.
A new correlate for intricate connections between fascial receptors, emotion, and self recognition
Introduction
What is interoception?
Sensual touch
A new phylogenetic development
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine