KATIE BYL, PhD, NANCY N. BYL, PT, MPH, PhD, FAPTA, MARTEN BYL, PhD, BRADLEY W. STOCKERT, PT, PhD, SEBASTIAN SOVERO, MS, CLAYTON D. GABLE, PT, PhD and DARCY A. UMPHRED, PT, PhD, FAPTA After reading this chapter the student or therapist will be able to: 1. Summarize the need, demand and principles for integrating advanced robotic technology in neurological rehabilitation. 2. Define common terminology used in the field of rehabilitation robotics and technology. 3. Classify the different types of advanced technology used in neurorehabilitation. a. Rehabilitation robots and assistive technology including: i. Service robots for movement ii. Service robots for physical assistance and indoor and outdoor navigation iii. Nonwearable robotic assistive device for mobility, unweighting, and object manipulation iv. Wearable robotic assistive device for upper-limb object manipulation v. Wearable robotic assistive device for lower-limb mobility and gait training vi. Communication robotics to enable interpersonal interaction vii. Interactive entertainment robotics for companionship and emotional support b. Advanced clinical technology including: i. Virtual reality training systems for improved neural recovery of upper- and lower-limb function ii. Computerized learning-based gaming systems for home training of individuals with physical disabilities and memory impairments iii. Computerized patient simulators for teaching clinical diagnoses and intervention strategies to medical professionals iv. Computer technology for teaching home exercise programs to patients 4. Use the guidelines for integrating robotics and assistive technology into a patient’s rehabilitation program. 5. Summarize the challenges and basic engineering principles involved in creating rehabilitation robotics and interfacing with advanced technology to help individuals to design: a. Robots that operate independently b. Controllers, actuators, and sensors required for service and assistive rehabilitation robots c. Human interfaces (physical, sensory physical, cognitive, and brain machine) d. User-friendly interfaces and controllers to maximize kinematics (e.g., force, velocity, timing) e. Rehabilitation robotics based on the materials and control technology currently available f. Safe robotics for rehabilitation 6. Discuss the benefits of performing a cost-effectiveness analysis when considering the application of robotic technology in rehabilitation. 7. Describe the challenges of commercializing robotic devices. 8. Discuss the future of advanced technology and rehabilitation. The objective of rehabilitation technology is to empower clinicians and individuals to take responsibility and control of the environment, facilitate physical and cognitive recovery, and comply with learning-based practice to drive neural adaptation and neural reorganization. The principles underlying technology and rehabilitation are summarized in Box 38-1. Since the early 1990s, medical science has been able to minimize damage to the nervous system postinjury. It is known that the central nervous system (CNS) possesses the potential for spontaneous healing and recovery. Learning-based sensory and motor training can be used to drive recovery of function. Rehabilitation robotics are a logical addition to supervised, one-on-one therapeutic interventions.1–9 BOX 38-1 Goals for advanced technology and rehabilitation robotics include the following: A Indirectly augmenting functional independence of individuals with impairments by: 1. performing mobility tasks for individuals at the home (e.g., using automatic motorized wheelchairs to move individuals from room to room; transitioning individuals from bed to chair and from chair to standing; moving patients who are standing; smart houses; calling for help) 2. minimizing the need for assistance from another individual 3. performing functional activities of daily living (ADLs; e.g., getting objects, cooking food, doing dishes, bathing, transferring) 4. helping perform difficult or repetitive tasks at work (e.g., assembly line tasks; lifting and moving heavy objects) B Directly improving human motor skill capabilities of individuals with impairments to enable them to: The objectives of assistive rehabilitation robotic devices need to be clearly defined in terms of: A unweighting a limb to reduce patient effort required for movement B actively canceling mechanical limitations on movement of the patient and robot arm dynamics (e.g., friction, inertia, and weight under gravity) C gently and progressively moving a limb to assist patient effort to perform a task D stabilizing a joint to enable a patient to produce a controlled movement E assisting the patient to improve the accuracy and quality of a movement F assisting the sequencing of movements Robotic technology for rehabilitation needs to be defined by: A location of the control system relative to the patient (controlled at a distance from the user [e.g., Web, Skype]), controlled in proximity to the user [e.g., by a therapist or engineer], or controlled by the user [e.g., wearable device or interface]) B environmental connection of the device and the patient (fixed to a nonmobile surface [e.g., wall], attached to a mobile platform [e.g., wheelchair], freely mobile with the patient [wearable]) C type of control system (e.g., joystick, sensor, breath) D type of interface (physical, sensory, cognitive, brain) E type of anatomical connection (e.g., by end effector only, end effector and multiple points of attachments with serial links or temporal links) Brain controlled interface rehabilitation robotics must be: Robotic technology can provide service, unweighting, passive assistance, active assistance, variable and on-demand assistance, or a combination of service and assistance.10 Computerized and robotic technology provides the foundation for patients to practice and attend to purposeful, goal-oriented, progressive tasks spaced over time. This technology can also minimize the risk of injury during retraining. Robotic interfaces, actuators, and controllers can convert sensory, physical, and cognitive signals to control robots, permit perception of spatial relationships, mobilize individuals in space, assist in object manipulation, provide emotional support, and allow individuals to call for help and communicate with others. In addition, through creative virtual training environments and gaming technology, patients can improve memory, motor skills, and movement quality. In addition, patient simulators can help medical professionals learn diagnostic processes, treatment interventions, and manual techniques. Computer-assisted technology can also improve our ability to teach home exercise programs to patients. Over the next 10 years, robotic technology will expand the opportunities for clinicians to assist patients to achieve maximum independence and quality of life with less dependence on others. The idea of interfacing technology with rehabilitation was introduced into practice by George J. Kelin in the 1940s. Kelin was a productive inventor from Canada who invented the power wheelchair for patients with quadriplegia, the microsurgical staple gun, and a wide range of industrial gearing systems. He also contributed to internationally important innovations in aviation and space technology. During the early 1970s, a new field emerged known as mechatronics, which combines mechanical, electrical, and control engineering design principles to produce a diverse range of useful practical devices.11,12 The science of biomechatronics then developed as a unique engineering discipline responsible for integrating neuromusculoskeletal appliances with biological systems to control and facilitate human-machine interactions as well as developing interfaces, sensors, actuators, and energy supplies to create functional devices for human use.13 The first conference on rehabilitation robotics was held in 1990. There are now multiple conferences each year on rehabilitation robotics. In 1999 the Robotics and Automation Society created the Rehabilitation Robotics Technical Committee to improve definitions and understanding about rehabilitation and assistive robotics.14 The scope of this technical committee has been recently specified as rehabilitation and assistive robotics. This modification is the direct outcome of the scientific progress and maturity reached in this broad research area. The goal of rehabilitation robotics is to investigate the application of robotics to therapeutic procedures for achieving the best possible motor, cognitive, and functional recovery for persons with impairments associated with aging, disease, or trauma (e.g., stroke, neuromotor disorders, brain trauma, orthopedic trauma, cognitive disease). Some clinicians have been skeptical of robotics in rehabilitation. Some health care providers worry that robots will replace therapists; others worry that robots are unsafe.8 However, researchers have persisted in developing innovative hardware, new control strategies, improved compliance, and feed-forward and adaptive control systems, as well as computerized modeling. In addition, new assistive, wearable robotic arm devices have been developed (e.g., MIT-Manus, the MIME, the ARM, and the iARM) to more carefully outline and address the engineering challenges related to what the robot can do, the logical physical targets for active assistance, and the joints and the types of movements that can safely be assisted. The field of rehabilitation robotics is still considered to be in its infancy. However, with the increasing demand for effective rehabilitative strategies, many new and exciting innovations are being developed. There are many robotic systems in various stages of research and development, but only a few are commercially available. Improvements in engineering, materials, human physical interfaces, software, and robotic designs will require constant analysis and adjustment in the future. It is projected that the market for personal robotic devices will be worth $15 billion by the year 2015.15,16 The challenges of robotic engineering are broad. Clinicians will need to participate in research to help document cost-effective outcomes as well as to develop efficient screening criteria to match patient needs with available robotic devices. One of these challenges will be to bridge the gap between the mechanical attributes of robotic sensors, actuators, controls, microprocessors, force, velocity, friction, unweighting, pressure tolerance, software design, and flexibility with the human limb, brain, and nervous system. Important issues related to safety, materials, technology, and the quality of matching machine and human movements must constantly be considered. These engineering issues are discussed later in this chapter. There is a variety of ways to classify computerized technology for rehabilitation. For this chapter, we will group robotic technology first in terms of how robotics are used with or by the client relative to rehabilitation. This classification system is summarized in Figure 38-1 and Box 38-2. Rehabilitation technology can be further classified by a variety of variables summarized in Box 38-3. Rehabilitation robotics can also be classified by type of interface used. Some classification systems classify technology by multiple parameters. Service robots usually focus on task performance, movement assistance, and stability. These devices can be fixed, can be movable, or can be attached to a wheelchair (Box 38-4). Assistive robotic devices help patients perform a task with direct or indirect assistance. Some of the assistive robotics are nonwearable but assist through unweighting or movement assistance (Box 38-5). Wearable robotics are specifically designed to be worn by patients to assist movements. These are designed for the upper or lower limb (Box 38-6). There are some new assistive training devices for the spine such as the Valedo Shape, Valedo Motion, and Hocoma devices (Figure 38-2). Prosthetic devices help patients maintain function despite the loss of a limb. Vocational robotics can enhance performance at work either in terms of repetitive motions or high-force task production that would otherwise be dangerous to humans. Communication robotic devices are designed to improve communication potential for subjects who cannot adequately speak or hear. Emotional support robotics are designed to provide emotional support for isolated individuals at home. BOX 38-5 VR training technology (with and without robotics) provides the opportunity to simulate simple and complex environmental and clinical situations to facilitate learning (Box 38-7). Game-oriented computerized learning systems are currently popular for fun and recreation, but they can also facilitate memory as well as sensory and motor skill development. Finally, computerized technology can also enhance teaching home exercises to patients. BOX 38-7 In this chapter, we will not address prosthetics for amputees, vocational robotics, communication robotics, emotional support robotics, or socially assistive devices,17,18 as these areas are considered specialty oriented and may or may not be included in traditional neurorehabilitation programs coordinated by physical or occupational therapists. However, information about the impact of the sound of the robot voice on patient motivation and compliance may be relevant to effectiveness. It is also important to acknowledge there are a number of motorized chairs, lifts, and walkers available that can be used to transition a patient from sitting to standing, or provide unweighting while walking or working on balance. Examples can be found in Box 38-8. Many of these systems are electromechanical systems controlled by the patient or the therapist. These devices are not usually programmable and are not classified as “rehabilitation robotics” or “advanced technology.” However, these types of devices are very beneficial for helping patients maintain walking and training to improve safety and quality of gait at home and with supervision. It is important for therapists to be sure these types of assistive devices have been integrated into a patient’s rehabilitation program and at home before recommending more sophisticated technology. Service robotics assist individuals with severe disabilities. Most commonly, the robot performs everyday activities (e.g., assisting with eating, drinking, object replacing, ambulating). There are three main types of schemes: desktop-mounted robots, wheelchair-mounted robots, and mobile autonomous robots. In general, these robots are used in the home, are interconnected to a variety of control systems, and are programmed to the environment and consequently are not very portable.19–21 Several examples of service robotics are described in Box 38-9.22–30 A major issue is patient control options for service robotic devices. For example, through the use of headpieces on robotic devices, information can be detected from flexion and extension, rotation, and side bending of the head to operate wheelchairs, TV sets, telephones, doors, and security systems. There are also some new interfaces that are sensitive to facial movements and optoelectronic detection of light-reflective head movements.31 Other interfaces are sensitive to eye movements or use voice recognition, brain control,32,33 and gesture recognition.34 These interfaces not only may allow control of the robot but also may be applied to move a limb or perform a task. BOX 38-9 I. Fixed upper-extremity service robotic devices A The earliest robots were fixed-site robots. B Fixed robotics were located in a nonmovable workstation. 1. The arm was preprogrammed to carry out selected routines which the user selected by pressing appropriate buttons (e.g., Seamone and Schmeisser at Johns Hopkins University, l974). 2. These workstations led to early Desktop Vocational Assistive Robots C Stanford University researchers, Boeing, and researchers responsible for several advances in France made significant improvements, particularly in integrating existing robotic systems. D Later, special manipulators were constructed to better fit the environment and the task. E The most well known systems for feeding were the Handy 1, My Spoon, and Neater Eater.22 F Today, these devices have been advanced with powered programmable devices (devices can provide maximum control for those with minimal voluntary ability and assistance for individuals who are trying to retrain the arm to work in a functional task). II. Mobile service upper-limb robots A Mobile service upper-limb robots are actually mechanical slaves. They are instructed to perform tasks. B The technology must be adequate to operate autonomously. C These units are expensive both in development and maintenance and usually require an engineer to set them up in the house and maintain their function over time. 1. The best known was developed in California at Stanford (the MoVAR system).23 2. This has a mobile base and a console to give feedback to the user to improve control. 3. The HelpMate robot is another mobile service robot that a disabled person can use to carry things from one place to another. If there is a cluttered environment within the home, that external environment negates the practical use of this robot. 4. The KARES II robot system24 uses a visual server to help provide assistance with movement (e.g., an eye mouse and a haptic suit with the arm mounted on a remote-controlled mobile base). 5. The Wessex robot allows different tasks to be performed in different rooms. III. Wheelchair-mounted upper-extremity manipulators A Wheelchair-mounted manipulators were first designed at the VA Prosthetics Center in New York (1984). 1. This sophisticated wheelchair-mounted manipulator is able to reach from the floor to the ceiling. 2. It has 7 degrees of freedom and a gripper hand. 3. This device may be sold to a rehabilitation facility to enable training of multiple users at that site. It is also sold to individual users. It is relatively expensive. B The Raptor25 was produced at a lower cost (only 4 degrees of freedom). C Exact Dynamics has also created a robotic manipulator (iARM) that is designed to help provide independence to people with severe disabilities. D Exact Dynamics also produces the Dynamic Arm Support (DAS), which compensates for the forces of gravity, making the arm practically weightless. These devices are currently being used in rehabilitation settings for training and for research. IV. Automatically guided wheelchairs (agws) A Powered wheelchairs can have autonomous intelligence systems attached. B AGWs are service rehabilitation robots intended to move the individual with severe disability. C Computer sensing devices can be set up to handle emergencies and assist with task performance. D The robot must receive instruction about the destination point. 1. These work best in a fixed, predictable environment and operate on an information decoding system whereby sensors identify the position and compare that position to the destination. 2. The algorithm must create a collision-free path from the starting point to a target. 3. Some robotic devices detect location and perform object avoidance behaviors through the use of ceiling-mounted or doorframe-mounted cameras. 4. In some cases the user may be able to modify the environmental situation by programming in new obstacles. V. Rehabilitation service robots: smart house design A For individuals with physical disabilities and older individuals, these smart devices allow residents to live independently with minimal or no human assistance. B There are a number of smart devices that can be installed in the house that are linked to one another to process information from the inhabitant to make decisions and take actions in case of emergency. C Smart house designs continue to be an area of development, particularly with the increasing number of aged individuals who are no longer able to manage independently. 1. One example is the Robotic Room developed at the Sato Laboratory of the Research Center for Advanced Science and Technology in the University of Tokyo.26 2. The Robotic Room consists of a ceiling-mounted robot arm (long-reach manipulator) and an intelligent bed with pressure sensors for monitoring the person’s posture. a. Modules monitor respiration without attachments. b. Cameras detect positions of the ends of the quilt on the bed. c. There is a second robot that is mobile to perform transportation tasks. The cameras on the ceiling detect robot positions. d. The interface of the robot consists of three ceiling-mounted video cameras to detect orientation of the user’s hand. When the user points at the robot, the television, curtains, and so on will be controlled. VI. Functional integration of multiple robots in the intelligent home environment A In the intelligent home environment, there are additional rehabilitation robotics designed to work with home-installed devices. B Placed in the correct arrangement, these robotic devices are controlled in a coordinated manner. 1. The M3S (multiple master–multiple slave) is a communication robot installed in the home. 2. This robotic system started with the TIDE Project27–29 and has set the standard for this type of robots. 3. Users can assemble a specific complete modular system. 4. In case of emergency, the user can halt the operation of the whole system (“dead man switch”). 5. The ICAN Project (Integrated Control for All Needs) developed the functional integration aspects of the system.23 6. The main objective is to propose an optimal control over all home-installed devices by a single interface device (e.g., joystick or switch input). 7. ICAN is a collaborative project in Europe and continues to receive government support.30 There is a variety of nonwearable assistive robotic devices. Some of these nonwearable assistive robotic devices are summarized in Box 38-10.35–43 This group of robotic devices primarily includes powered wheelchairs with autonomous intelligence, body-weight–supported mobile walking aids, robots for body support with indoor and outdoor navigation, hands-off service robotic devices, and body-weight–supported treadmill systems (BWSTSs) with and without robotics.37,41–45 BOX 38-10 I. Body-weight–supported mobile walking aids A Newly designed rehabilitation robotic systems can function as walking aids to help those who cannot walk independently. B Some mobile walking aids can walk the client, but others can also be used for training the patient to walk. 1. There are several electric motor-based gait rehabilitation systems. 2. Generally, gait rehabilitation systems include a robotic manipulator, a mobile platform, and a sensor system. 3. The robotic manipulator controls the amount of body-weight support. 4. The robot is mounted on a mobile platform that not only can support the user’s weight but can be adjusted to the height of the subject and provide stability when walking. 5. The robot has sensors to detect the status of the user (direction and velocity). 6. The mobile platform moves the whole system according to the subject’s motion with objects in the way of the moving platform detected by ultrasonic sensors on the front of the system.43 a. The mobile platform can vary from having a carlike design to having a mobile base with driving and steering wheels and differential driving mobile bases. b. The front-wheel-drive carlike model has a complex mechanical design and can be very expensive. c. The synchronous driving and steering mechanisms are complex but can approximate human walking, especially when the path is not linear. d. Differential driving mechanisms require two independent driving wheels. e. The mechanical architecture is simple and practical to implement but may require more maintenance. f. There are training and following modes. g. The challenge is to have sensors that can control stop and go of the user. h. The supervisor can push an emergency stop button, but if the user is generally weak and does not have adequate balance reaction, the patient could fall when the mobile unit stops suddenly. i. Example: the gait rehabilitation system: (a) Used to study the impact of unweighting on gait parameters and patient exertion and heart rate.37 (b) Researchers have demonstrated that with increasing amounts of unweighting, there is an increase in single leg support and a decrease in double leg support, in terms of the percentage of time a given leg contacts the ground during steady-state walking. (1) At 0% unweighting, single leg stance was 34.5%. (2) At 20% unweighting, single leg stance was 38%, with 23% on both limbs. (3) At 40% body unweighting, single leg stance was 42.5%, and 17.5% of time included bilateral support. (c) With increased unweighting and comfortable walking speed, there is a decrease in heart rate. C If the device is primarily used to facilitate standing to prevent contractures and skin ulcers, it may be classified as a stander rather than a walking aide. II. Robots for physical support 1. These devices assist users with limb and trunk weakness and visual impairments; usually the patients are older. 2. These machines usually have a motorized base to give physical support to the user. 3. The robot control system identifies its specific location and puts out voice synthesized navigation instructions or warnings about obstacles on the intended routes. 4. The robot automatically detects the user intention regarding walking speed and direction of movement. 5. Examples include the HITOMI,38 the PAM-AID,39 and the WHERE (walking and moving helper robot system).37 B Indoor and outdoor navigation 1. These devices provide physical support for unweighting, harness or robotically controlled protection from falling, and the ability to step. 2. The robot protects against falling when the end-range body sway has been exceeded. 3. These devices are best for improving postural righting reactions without falling. C Unweighting with robotic-controlled stepping 1. These devices can include harness support and unweighting while the user stands on an electromechanical platform system. 2. The feet are attached to assistive computerized devices that force stepping of the feet. 3. Training is done on the device (e.g., electromechanical gait trainer developed by Hesse). 4. With practice in stepping, the goal is to improve efficiency and effectiveness of walking. 5. Studies with this device confirm it is safe and there are improved outcomes as measured by increased walking speed and endurance. D Unweighting with robotic-controlled destabilization 1. One device that has been tested at the University of Chicago is the KineAssist (IMAGE).40 (See Figure 38-6.) 2. The KineAssist is a robotic gait training device that emphasizes balance recovery training during gait training. 3. The goal is to provide partial body-weight support and postural control on the torso while the patient walks over ground. a. This device is on a mobile, multidirectional base that allows the patient to walk over ground, indoors or outdoors. b. The trunk and pelvis are free to move, the legs are accessible, and the arms are free. c. A servomotor follows the patient in forward, rotation, and sideways walking. d. It has a robotic arm that is linked to the patient’s trunk. e. The robotic arm can be set to allow the patient to move easily and even exceed the limit of stability. f. The robot can also be programmed to specifically interfere with stability. g. The patient can lose balance and “fall,” but the robotic arm will stop the fall after a defined range. h. The patient can experience what is needed to keep from falling when the limit of stability has been reached. i. With practice the patient can improve postural righting and balance. A These are devices that can be placed on the less affected side to restrict motion of a limb. B The objective is to force the patient to use the affected limb (similar to constraint-induced therapy in which the least-affected limb is constrained with a mitt or a cast; see Chapter 9). C Usually the robot is programmed to perform specific tasks with the patient assisting. D The robot could give feedback by nodding, talking in a synthesized voice, or using a prerecorded friendly human voice with humor and engagement that could be matched to some extent to the patient’s personality. E Patients appear to perform better when they receive a robot voice for feedback and the robot personality is matched to the patient.
Integrating technology into clinical practice in neurological rehabilitation*
Introduction to the application of robotics and technology in rehabilitation
General overview
 PRINCIPLES SUPPORTING ADVANCED TECHNOLOGY AND REHABILITATION ROBOTICS IN NEUROREHABILITATION
PRINCIPLES SUPPORTING ADVANCED TECHNOLOGY AND REHABILITATION ROBOTICS IN NEUROREHABILITATION
History supporting the use of technology in neurological rehabilitation
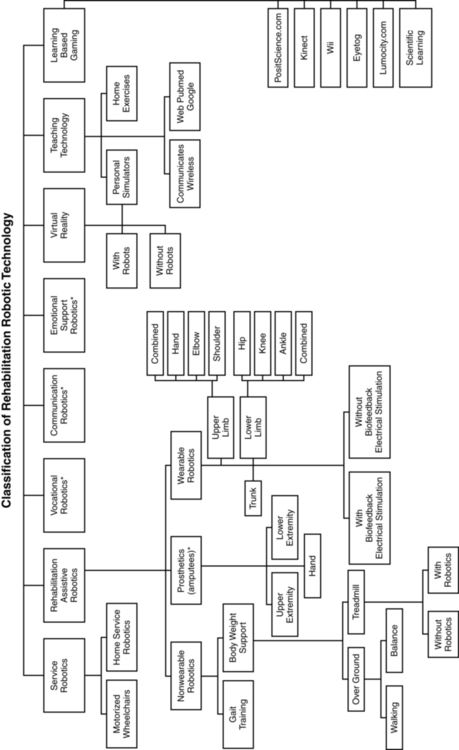
Classification of rehabilitation robots
General principles
 TYPES OF NONWEARABLE ASSISTIVE ROBOTIC DEVICES
TYPES OF NONWEARABLE ASSISTIVE ROBOTIC DEVICES
 Body-weight–supported mobile walking aids
Body-weight–supported mobile walking aids
 Robotic devices for physical support (indoors, outdoors)
Robotic devices for physical support (indoors, outdoors)
 Robotic devices for physical support, unweighting, and mechanical stepping in place
Robotic devices for physical support, unweighting, and mechanical stepping in place
 Robotic devices for unweighting and controlled destabilization
Robotic devices for unweighting and controlled destabilization
 Robotic devices for unweighting and gait training
Robotic devices for unweighting and gait training
 Robotic devices for unweighting and robotic stepping on a treadmill
Robotic devices for unweighting and robotic stepping on a treadmill
 EXAMPLES OF HOW VIRTUAL REALITY CAN ASSIST LEARNING
EXAMPLES OF HOW VIRTUAL REALITY CAN ASSIST LEARNING
Description of robotic systems by type
Service robotic systems that provide movement assistance
 SUMMARY OF SERVICE ROBOTICS
SUMMARY OF SERVICE ROBOTICS
Assistive robotics
Nonwearable assistive robotic devices.
Types of nonwearable assistive robotic devices.
 NONWEARABLE ASSISTIVE ROBOTIC DEVICES FOR GAIT TRAINING
NONWEARABLE ASSISTIVE ROBOTIC DEVICES FOR GAIT TRAINING
Related posts:
![]() Multiple sclerosis
Multiple sclerosis
![]() Contemporary issues and theories of motor control, motor learning, and neuroplasticity
Contemporary issues and theories of motor control, motor learning, and neuroplasticity
![]() Electrophysiological testing and electrical stimulation in neurological rehabilitation
Electrophysiological testing and electrical stimulation in neurological rehabilitation
![]() Orthotics: evaluation, intervention, and prescription
Orthotics: evaluation, intervention, and prescription
![]() Traumatic spinal cord injury
Traumatic spinal cord injury
![]() Neonates and parents: neurodevelopmental perspectives in the neonatal intensive care unit and follow-up
Neonates and parents: neurodevelopmental perspectives in the neonatal intensive care unit and follow-up
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






























 ed (
ed ( pper •imb)
pper •imb)














 ’ Go wa•ker
’ Go wa•ker

