Abstract
Purpose
To compare the individual influence of different types of socket designs on the hip’s range of motion in transfemoral amputees.
Patients and methods
We studied the kinematic parameters of the hip joint for patients with transfemoral amputation under four experimental conditions: without a socket, with a quadrilateral socket, an ischial containment socket, an ischial-ramal containment socket. An opto-electronic system was used to record the movements in the frontal and sagittal planes for a 3D movement analysis.
Results
The hip’s range of motion is always significantly restricted with the sockets, regardless of their type, compared to the situation without a socket ( P < 0.05). The adduction and extension movements are the most restricted. The global amplitude (i.e., the sum of all the ranges of motion) is significantly higher for the ischial-ramal containment socket (139.5°) compared to the ischial containment socket (125.4°, P = 0.002) and the quadrilateral socket (127.3°, P = 0.01). No comparable study exists in the literature, especially for the ischial-ramal containment socket.
Conclusion
The ischial-ramal containment socket seems to be the most interesting type of socket in terms of the criterion studied. It still remains to identify the possible functional improvements that this design would provoke during gait and during daily activities.
Résumé
Objectif
Comparer l’influence isolée de différents types d’emboîture sur les amplitudes articulaires de la hanche de l’amputé transfémoral.
Patients et méthodes
Nous avons étudié les paramètres cinématiques de l’articulation de la hanche chez quatre patients amputés transfémoraux dans quatre conditions : sans emboîture, avec emboîture quadrangulaire, à ischion intégré et à branche ischiopubienne incluse. La capture des mouvements a été enregistrée dans le plan frontal et le plan sagittal par un système optoélectronique 3D d’analyse du mouvement.
Résultats
Les amplitudes articulaires de la hanche sont toujours significativement limitées avec les emboîtures, quel que soit leur type, par rapport à la situation sans emboîture ( p < 0,05). Ce sont les mouvements d’adduction et d’extension qui sont les plus limités. L’amplitude globale (somme des amplitudes) est significativement supérieure pour l’emboîture à branche ischiopubienne incluse (139,5°) comparée à l’emboîture à ischion intégré (125,4°, p = 0,002) et à l’emboîture quadrangulaire (127,3°, p = 0,01). Il n’existe dans la littérature aucune étude comparable, faisant notamment référence à l’emboîture à branche ischiopubienne incluse.
Conclusion
L’emboîture à branche ischiopubienne incluse est celle qui paraît la plus intéressante sur le critère étudié. Il reste à mettre en évidence l’amélioration éventuelle qu’elle apporterait à la marche et en situation écologique.
1
English version
1.1
Introduction
The gait of unilateral transfemoral amputees has already been studied by many authors . These studies are based on physiological data, such as oxygen consumption, or kinematic data from kinematic or goniometric techniques. Kinematic parameters are thus the evidence of the total integration of a prosthesis in the new gait pattern imposed by the absence of the limb.
A leg prosthesis is traditionally composed of three components: the foot, the knee, and the socket. Van Der Linde et al. conducted a systematic review of the literature on the contributions of these components. The associations and interactions of these components determine the way in which the patients are going to use their prostheses in daily life: while walking, standing upright, sitting, going up/down stairs, and changing from a sitting position to a standing position. Several authors have shown that, for non-amputees, the functional capacities of the hip joint determine the efficiency and the comfort of these activities.
The socket is the part of the prosthesis that interacts with the stump. It has the functional objective of transmitting the movements of the residual limb to the prosthetic elements, despite skin sliding or the piston effect. Like the prosthetic feet and knees, the socket has benefited from customary research and innovation . At the beginning of the 1980s, Long developed ischial containment sockets; until then, the quadrilateral sockets were the sockets the most commonly used. An ischial containment socket envelops the ischium; in the quadrilateral socket, the ischium presses vertically on the sub-ischial shelf . Sabolich suggested that the ischial containment socket, unlike the quadrilateral socket, aims to put the femur into the adduction position. This position should allow gait efficiency to be improved through gluteus medius muscle action. The X-ray-based measurements taken by Hachisuka et al. confirm the femur is more in the medial position using the ischial containment socket.
Several studies have used subjective evaluations to compare the ischial containment sockets to the quadrilateral sockets. Flandry et al. used questionnaires and found that the subjective evaluations of patients approve the ischial containment sockets for comfort, balance and prosthesis control. Hachisuka et al. also reported a better subjective comfort for ischial containment sockets, especially in the sitting position. Unlike these studies, Boonstra et al. found that the evaluation of the quadrilateral sockets was better than that of the ischial containment sockets.
In terms of the comparison of physiological parameters, Gailey et al. showed a reduced energy consumption while walking, using an ischial containment socket instead of a quadrilateral socket. These results confirm the results of Flandry et al. , who also noticed an improvement of the metabolic cost of walking, as well as a reduction of the trunk’s lateral compensation movements, with an ischial containment socket. However, the most recent study by Hachisuka et al. did not reveal a significant difference in the metabolic output while walking in relation to the socket used. Taking different walking speeds into account suggests that the advantage of the ischial containment socket is demonstrated at high walking speeds .
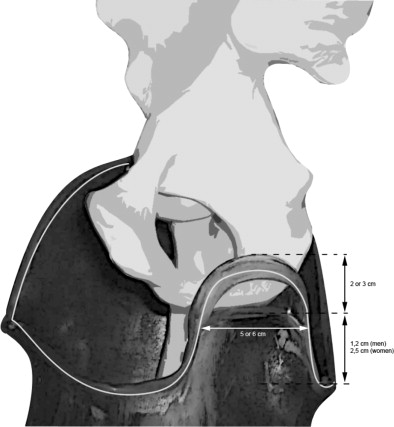
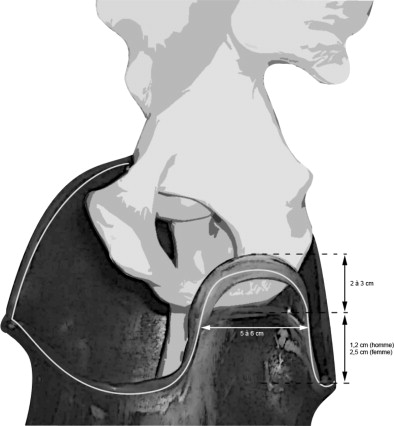
Marlo Ortiz modified the concept of the ischial containment socket and proposed the ischial-ramal containment socket, also called the Marlo Anatomical Socket (MAS ® ) ( Fig. 1 ). This socket no longer envelopes the ischium, but rather the ischio-pubic ramus. The ischio-pubic ramus containment surface rises 2 or 3 cm over the ischio-pubic ramus. Its width is 5 or 6 cm. The medial edge is under the ischio-pubic ramus. The anterior trim line is positioned at the level of pubic ramus and then rises to 0.6 cm under the anterior superior iliac spine; it follows the inguinal fold to link with the lateral wall, which includes trochanter. At the posterior level, the median point in the form “U” is positioned 1.2 cm under the ischio-pubic ramus for men and 2.5 cm for women. Laterally, the form “U” joins the external wall.
In the literature, we did not find studies investigating this new type of socket, although Hagberg et al. underlined the advantages of doing so in 2005. Still, this new type of socket is relatively recent in terms of the transmission speed of new techniques in orthopedics, especially since its production is complex, involving human and material costs that are now poorly valorized.
The hip is the vector transmitting the forces from the patient to his/her prosthesis, and measuring the range of motion in the hip is a good way to quantify the patient’s incapacities . For this reason, we chose to study specifically the hip’s range of motion in order to determine which socket is the least restrictive. In order to identify the influence of a prosthesis component, one of these components can be modified without modifying the others or one of these components can be studied independently of the others . In our research, we studied the individual influence of the different types of sockets on the hip’s active range of motion in transfemoral amputees.
1.2
Patients and methods
We used 3D movement capture technology to compare the influence of the various sockets on the hip’s range of motion in transfemoral amputees.
1.2.1
Studied population
The population was composed of four male patients, with an average age of 51 years, who all were unilateral transfemoral amputees for at least 5 years. Three cases were traumatic amputations, and one case was a vascular amputation. They all wore their prostheses daily, at least 8 hours per day. Three patients had an ischial-ramal containment socket, and one had an ischial containment socket. These four patients participated in the study voluntarily. This research project was validated by the Comité de protection des personnes (People Protection Committee) at the University of Bordeaux A. Table 1 provides the patient characteristics.
| Subject | Weight (kg) | Height (cm) | Age (years) | Stump length (cm) | Controlateral crural segment length (cm) | Shortening (%) |
|---|---|---|---|---|---|---|
| 1 | 81 | 183 | 42 | 32.5 | 43.5 | 25.3 |
| 2 | 57 | 165 | 42 | 29 | 34 | 14.7 |
| 3 | 60 | 158 | 57 | 27 | 33 | 18.2 |
| 4 | 80 | 185 | 63 | 22.5 | 37 | 39.2 |
1.2.2
Socket production protocol
Each patient had the three socket types studied produced for them individually: a quadrilateral socket, an ischial containment socket, and an ischial-ramal containment socket. The thermoforming of the sockets was performed with Orthochoc ® plastic. The same tightness rating were used, as well as the same type of Stepline ® liners with distal attachment. All the modifications were performed by the same ortho-prosthetist, who was experienced and trained in various techniques.
1.2.3
Equipment
The tests were recorded using an Elite ® system (BTS, Italy), with 12 cameras functioning at 200 Hz.
1.2.4
Our model
We used a model with two articulated rigid solid segments, representing the residual limb and the pelvis, to measure the kinematics of the hip movements. A total of 10 retro-reflective markers were placed the body: three markers on the thigh, two markers on the left and right anterior superior iliac spine, two markers on the trochanters, one marker between the two sacral dimples, and two markers on distal attachment of the liner ( Fig. 2 ).

1.2.5
Measurement protocol
Four experimental conditions were used: without a socket, with a quadrilateral socket, with an ischial containment socket, and with an ischial-ramal containment socket. In order to neutralize the influence of the other prosthesis components (i.e., foot and knee), all tests were performed using only the socket. Active flexion-extension movements and active abduction/adduction movements were performed under the four conditions. The patients were asked to make the movements as ample as possible, while holding onto a fixed support (i.e., something similar to a bike’s handlebars), placed before them. The resting position of the residual limb in the different experimental conditions may fluctuate and thus cannot be used as the original position. For this reason, we preferred to use the vertical axis as our reference.
The joint amplitudes were calculated based on the movements, which continued for 30 seconds. These movements were repeated three times, with a rest period between each trial. The four experimental conditions were tested in a random order.
The patients were outfitted with a liner with distal attachment for all the experimental conditions. In fact, the tests performed without a liner in a pre-study showed us the significance of the deformations of the residual limb. These deformations cannot be taken into account in an articulated, rigid, solid system model of the coxofemoral joint. The liner allowed us to retain the soft tissues of the stump. Marks were traced on the liner to reproduce the positions of the retro-reflective markers during the four experimental conditions. The patients did not remove their liners between each socket change. The use of transparent plastic permitted the motion capture operator to place the retro-reflective markers on the socket in the locations of the marks on the liner.
1.2.6
Primary evaluation criterion
The primary evaluation criterion was the global amplitude of the hip. This parameter was calculated by adding the hip joint amplitudes for the various planes. Sochart and Porter used this parameter in their study. This parameter has the advantage of reflecting the hip’s mobility with a single value.
1.2.7
Measurement precision
Several articles have studied the precision of the motion capture systems for gait analysis . The errors generally reported for the “Helen Hayes” models are under 5°, but may be higher for the hips . The results obtained with our model during the pre-study show us that the root mean square (RMS) error for the hip movements is around 3°.
1.2.8
Statistical analysis
We used the Student test under Excel, with the additional analysis macros to highlight the significativity of the differences between the four experimental conditions. This is a one-sided test (superiority) with a threshold of significativity set to P = 5%.
1.3
Results
Table 2 gives the averages of the angular values of the different amplitudes in flexion, extension, abduction and adduction for the four patients. The measurements are given individually and then added two by two to obtain amplitude values in the sagittal and frontal planes. The measurements are reported without a socket and then for each type of socket. For each movement studied, the table also provides the percentage of amplitude loss compared to the reference amplitude measured without a socket.
| Averages | Flexion | Extension | Sagittal joint amplitude | Abduction | Adduction | Frontal joint amplitude | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F ± SD (°) | LF ± SD (%) | E ± SD (°) | LE ± SD (%) | FE ± SD (°) | LFE ± SD (%) | AB ± SD (°) | LAB ± SD (%) | AD ± SD (°) | LAD ± SD (%) | ABAD ± SD (°) | LABAD ± SD (%) | |
| Without a socket | 80.8 ± 13.1 | – | 16.6 ± 2.4 | – | 97.4 ± 15.5 | – | 46.4 ± 3.7 | – | 23.2 ± 1.9 | – | 69.6 ± 5.4 | – |
| With a ischial-ramal containment socket | 70.9 ± 13.7 | 12.2 | 14.2 ± 2.3 | 14.5 | 85.1 ± 15.7 | 12.6 | 34.8 ± 4.6 | 24.9 | 19.6 ± 0.7 | 15.5 | 54.4 ± 5.2 | 21.8 |
| With an ischial containment socket | 63.5 ± 12.7 | 21.5 | 11.3 ± 1.2 | 31.5 | 74.8 ± 13.9 | 23.2 | 38.1 ± 5.0 | 17.8 | 12.5 ± 1.1 | 46.2 | 50.6 ± 6.0 | 27.3 |
| With a quadrilateral socket | 64.5 ± 11.8 | 20.2 | 12.7 ± 2.5 | 23.1 | 77.2 ± 14.2 | 20.7 | 38.1 ± 4.5 | 17.9 | 12.1 ± 0.8 | 48.1 | 50.1 ± 5.2 | 28.0 |
Two strong tendencies are seen at this point. The first shows adduction is most restricted movement for the sockets tested, followed by extension. The second tendency indicates the ischial-ramal containment socket restricts the hip’s range of motion the least.
The small size of our population didn’t permit us to conduct multiple comparisons. We chose to restrict our study to the use of one single evaluation criterion – the global amplitude of the hip joint – defined as the sum of the angular values of each movement (i.e., flexion, extension, abduction and adduction). This parameter was calculated for four experimental conditions: without a socket, with a quadrilateral socket, with an ischial containment socket, and with an ischial-ramal containment socket. These results are provided in Table 3 .
| Averages | Sagittal joint amplitude | Frontal joint amplitude | Global amplitude | |||
|---|---|---|---|---|---|---|
| FE ± SD (°) | LFE (%) | ABAD ± SD (°) | LABAD (%) | GA ± SD (°) | LGA (%) | |
| Without a socket | 97.4 ± 15.5 | – | 69.6 ± 3.6 | – | 167.0 ± 20.8 | – |
| With a ischial-ramal containment socket | 85.1 ± 15.7 | 12.6 | 54.4 ± 5.2 | 21.8 | 139.5 ± 20.4 | 16.4 |
| With an ischial containment socket | 74.8 ± 13.9 | 23.2 | 50.6 ± 6.0 | 27.3 | 125.4 ± 19.6 | 24.9 |
| With a quadrilateral socket | 77.2 ± 14.2 | 20.7 | 50.1 ± 5.2 | 28.0 | 127.3 ± 18.8 | 23.8 |
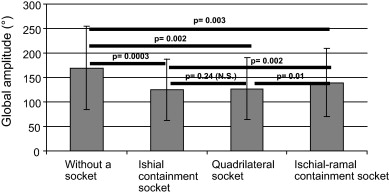
As shown in Fig. 3 , the statistical tests suggest the following significant differences:
- •
a reduction of the global amplitude of the hip joint, whatever the type of socket, compared to physiological conditions without a socket;
- •
a global amplitude of the hip joint less restricted by the ischial-ramal containment socket than the other two sockets;
- •
no significant difference between the ischial containment socket and the quadrilateral socket.
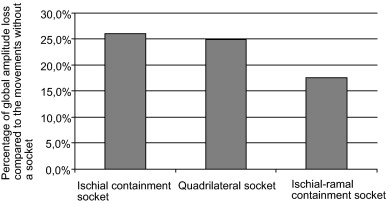
If the global percentage of amplitude loss under each experimental condition is analyzed ( Fig. 4 ), the ranking of sockets is identical: the ischial-ramal containment socket involves less restriction of the global range of motion compared to the ischial containment socket and the quadrilateral socket.
1.4
Discussion
This paper presents an evaluation method for the hip’s active range of motion in transfemoral amputees. This method uses a 3D motion capture system. The method’s precision is thus linked to the precision of the system. Stereo-photogrammetry is known to be sensitive to skin sliding in relation to marker placement and deformation of the soft tissues. These imponderable phenomena (i.e., skin sliding and deformation) are very important in transfemoral amputees.
In order to compensate for this critical aspect of the patient marker placement, we chose to use a liner, which permits us to limit the soft tissue deformation in the residual limb. We used this liner in all the experimental conditions, including the movements without a socket. We did not quantify the influence of wearing the liner on the patient movements. Thus, it is possible the results obtained with the liner but without the socket would be slightly different from the results for a patient performing the movements without a liner.
We tested the extreme joint amplitudes of the patients without the other prosthesis components. In this way, the results obtained are only determined by the socket type. In real life, the patients do not wear their socket independently of the other prosthesis components, but integrated in the whole prosthesis. If the same study was conducted with the whole prosthesis in place, it is highly likely that the results obtained would be different, notably because of the increased weight of the whole prosthesis. As a result, the joint amplitudes would certainly be reduced.
Our results show that the three socket types studies have a negative impact on the physiological functioning of the hip joint; however, the ischial-ramal containment socket restricts the movements the least significantly. This study has a population with only four participants, which did not allow us to statistically test several parameters, so there is a risk of a type 1 error, also known as a false positive.
Nonetheless, we identified some tendencies. One of them showed that adduction is the movement the most restricted by the sockets tested, followed by extension. Rotation movements were not investigated in the study, but it could be interesting to study them in the future in order to complete the data collected on the influence of the sockets.
As a parameter to analyze, this study does not take into account the length of the stump. Generally, only a little data is available on the influence of stump length in transfemoral amputees. For 11 patients using three different types of knees, Jaegers et al. reported an increased length of the stance phase on the healthy leg for any decrease in the stump length. For 13 patients, Baum et al. did not find any influence of the stump length on any of the studied parameters (i.e., gait speed, cadence, stride length on either the healthy side or the prosthetic side, stance phase length on both sides, hip flexion, lateral or anterior trunk inclination) for stumps that had lengths between 57% and 100% of the controlateral crural segment length. For 12 patients whose stumps had an average length of 70% of the controlateral crural segment, Haschisuka et al. did not find any significant differences in the oxygen consumption while walking at a comfortable speed. Table 1 reports the stump lengths used in this study, which were between 60.8% and 85% of the controlateral crural segment length. Based on the available data, this parameter had little influence on our results.
We compared the various socket designs with the objective of determining their respective influences of the hip kinematics. Several authors have already this type of study , but no one has analyzed specifically the behavior of the hip joint. Frequently, these studies concern energy consumption or the feelings of the patients, and they compare only the quadrilateral socket to the ischial containment socket. Their results show a better patient satisfaction for patients who wear an ischial containment socket and a reduction of oxygen consumption while walking rapidly (over 3 km/h) .
All these studies, most of them done in a laboratory setting and studying global phenomena, underline a real incertitude as to the interest of the patients to use one socket design rather than another in everyday life. In our study, we chose to focus on a simple task: the hip joint’s movement in interaction with a socket. In fact, the socket is the only component in direct contact with the patient’s body, and it conditions the functioning of the other prosthesis components when using the prosthesis. Any decrease in the range of motion at this level will have repercussions in the daily life of the patients .
In 1970, Johnston and Smidt studied the hip joint of non-amputees in their daily lives. After hip surgery, it was necessary to recover a flexion of 120°, an abduction of 20° and an external rotation of 20° to allow normal functioning of the hip joint (e.g., putting on shoes, sitting down on/getting up from a chair, picking up an object). Extending the hip makes it possible to walk with a normal stride length .
Hagberg et al. studied the hip’s range of motion in transfemoral amputees with and without a socket, as well as the subjective feeling of comfort in a sitting position. They compared 43 patients with prostheses equipped with quadrilateral or ischial containment sockets to 20 patients whose prostheses were fixed directly in the bone by osteointegration. With the prosthesis in place, the results show a reduction of the hip’s range of motion in all directions for the “socket” group compared to the “osteointegration” group; however, there were no significant differences between the two types of socket. The reduction was more noticeable in flexion (−15°). In the saggital plane, the total loss of flexion-extension was 24°, while in our study, it was 22.6° for the ischial containment socket, 20.2° for the quadrilateral socket, and 12.6° for the ischial-ramal containment socket. Thus, our results for the first two sockets are confirmed by those of Hagberg et al. .
A study by Boonstra et al. highlights the importance of preserving good hip mobility. They reported a significant correlation between the hip’s sagittal amplitude, flexion-extension, and walking speed. The less the joint is restricted, the more the walking speed increases. Similarly, in the study by Burger et al. , on passing from sitting position to a standing position, the amputees need a maximum range of motion in flexion; otherwise, the action is longer and the compensations are more important.
In the end, all these studies show the advantages of making sockets that preserve the best possible hip mobility. In the sagittal plane, if there is more residual hip flexion, the sitting position is more comfortable, the patient can get up more easily, and the walking speed is higher. Similarly, it is necessary to minimize the direct contact of the ischium and socket in order to promote the posterior stride. In our study, the ischial-ramal containment socket responds better to this objective in the experimental conditions described, probably because of its very specific cuts and volumes. However, it is important to relativize the universality of this socket’s indication because it requires leaning on the ischio-pubic zones, which can influence the tolerability using this type of socket. Our results are the first that show the advantages of using the ischial-ramal containment socket compared to the more traditional sockets.
Nonetheless, this study was performed in a laboratory setting, with a limited number of patients and with maximal range of motion. In future research, it will be important to study the advantages of this socket in the different daily living activities. We can deduce that it is not while walking that the benefit of this socket is the most important, since the necessary joint amplitudes are relatively limited. It would be while doing activities when the hip is more solicited that the socket would prove its worth: sitting position, passing from a sitting position to a standing position, going up/down stairs, and the ante-flexion movements in order to, for example, pick up an object. Other studies could be done with the objective of better targeting the indication of these sockets, which are and will remain difficult to produce.
1.5
Conclusion
Our research has shown the negative influence that all these sockets have on the correct functioning of the hip joint in transfemoral amputees. This loss of joint mobility probably decreases the patient’s quality of life. However, recent research on new concepts of cutting and form, especially the socket developed by Marlo Ortiz, called the ischial-ramal containment socket, allow us to hope for an improvement of this situation.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
2
Version française
2.1
Introduction
La marche de l’amputé transfémoral unilatéral a déjà été étudiée par de nombreux auteurs . Ces travaux se basent sur des données physiologiques comme la consommation d’oxygène ou sur des données cinématiques issues de techniques cinématographiques ou goniométriques. Les paramètres cinématiques sont alors le reflet de l’intégration d’une prothèse complète dans un nouveau schéma de marche imposé par l’absence du membre. Une prothèse se compose classiquement de trois parties : le pied, le genou, l’emboîture. Van Der Linde et al. ont effectué une revue de littérature systématique sur l’apport des différents composants. L’association et les interactions de ces éléments entre eux conditionnent la manière dont le patient va pouvoir exploiter sa prothèse au quotidien : au cours de la marche, en station debout statique, en position assise, en montée et descente d’escaliers et en transition assis-debout. Plusieurs auteurs ont montré que, pour des sujets non amputés, les capacités fonctionnelles de l’articulation de la hanche conditionnent l’efficacité et le confort de ces activités.
L’emboîture est la partie de la prothèse qui s’interface avec le moignon. Elle a pour objectif fonctionnel de transmettre les mouvements du membre résiduel aux éléments prothétiques et cela malgré les effets de glissement sur la peau ou de piston. L’emboîture a bénéficié, comme les pieds et les genoux prothétiques, de recherches et d’innovations régulières . Au début des années 1980, Long met au point les emboîtures à ischion intégré alors que, jusque-là, les emboîtures quadrangulaires représentaient la majorité des emboîtures utilisées. Une emboîture à ischion intégré enveloppe l’ischion alors que dans une emboîture quadrangulaire, l’ischion appuie verticalement sur la tablette sous-ischiatique . Enfin, contrairement à l’emboîture quadrangulaire, Sabolich indique que l’emboîture à ischion intégré a pour objectif de mettre le fémur en position d’adduction. Cela doit permettre d’améliorer l’efficacité de la marche par une action sur le muscle moyen fessier. Les mesures effectuées par Hachisuka et al. à partir de radiographies confirment une position du fémur plus en position médiale avec l’emboîture à ischion intégré.
Plusieurs études ont utilisé des évaluations subjectives pour comparer les emboîtures à ischion intégré aux emboîtures quadrangulaires. Flandry et al. utilisent des questionnaires et trouvent que l’évaluation subjective des patients est favorable aux emboîtures à ischion intégré pour le confort, l’équilibre et le contrôle de la prothèse. Hachisuka et al. rapportent aussi un meilleur confort subjectif pour l’emboîture à ischion intégré, en particulier en position assise. À l’opposé de ces tendances, Boonstra et al. trouvent que la cotation de l’emboîture quadrangulaire est meilleure que celle de l’ischion intégré. Concernant les paramètres de comparaison physiologique, Gailey et al. montrent une réduction de la consommation d’énergie à la marche en utilisant l’emboîture à ischion intégré par rapport à l’emboîture quadrangulaire. Ces résultats sont venus confirmer ceux de Flandry et al. qui notent aussi une amélioration du coût métabolique de la marche ainsi qu’une diminution des mouvements latéraux de compensation du tronc avec l’emboîture ischion intégré. Cependant, l’étude plus récente de Hachisuka et al. n’a pas révélé de différence significative du rendement métabolique à la marche en fonction de l’emboîture utilisée. La prise en compte des différentes vitesses de marche indique que l’intérêt de l’emboîture à ischion intégré se révèle dans les vitesses élevées .
Marlo Ortiz modifie le concept de l’emboîture à ischion intégré et propose l’emboîture anatomique à branche ischiopubienne incluse (BIPI) dite aussi emboîture MAS © pour Marlo Anatomical Socket ( Fig. 1 ). Ici, ce n’est plus l’ischion qui est enveloppé par l’emboîture mais la branche ischiopubienne. La palette de contention de la branche ischiopubienne monte de 2 à 3 cm au-dessus de la branche ischiopubienne. Sa largeur est de 5 à 6 cm. Le bord médial est en dessous de la branche ischiopubienne. La ligne de découpe antérieure se trouve au niveau de la branche puis remonte pour être à 0,6 cm sous l’épine iliaque antéro-supérieure, elle suit le pli inguinal pour se raccorder à la paroi latérale. Celle-ci englobe le trochanter. Au niveau postérieur, le point médian de la forme en « U » se trouve à 1,2 cm sous la branche ischiopubienne pour les hommes et à 2,5 cm pour les femmes. Latéralement, la forme en « U » rejoint la paroi externe.
Related posts:
 Comparative study of indices of activity evaluation in rheumatoid arthritis
Rehabilitation in patients with peripheral arterial disease
Dependent patients discharged home from PRM departments: Relevant indicators
Analyse de livre
Impact of a rehabilitation program on muscular strength and endurance in peripheral arterial occlusive disease patients
The Prevention of Foot Ulceration in Diabetic Patients
Comparative study of indices of activity evaluation in rheumatoid arthritis
Rehabilitation in patients with peripheral arterial disease
Dependent patients discharged home from PRM departments: Relevant indicators
Analyse de livre
Impact of a rehabilitation program on muscular strength and endurance in peripheral arterial occlusive disease patients
The Prevention of Foot Ulceration in Diabetic Patients
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


