, Paola Catalano1, Andrea Piccioli2, 3, Maria Silvia Spinelli4, 3 and Federica Zavaroni1
(1)
Anthropological Service, Soprintendenza Speciale per il Colosseo, il Museo Nazionale Romano e l’Area Archeologica di Roma, Rome, Italy
(2)
Oncologic Center “Palazzo Baleani” Azienda Policlinico “Umberto I”, Rome, Italy
(3)
The Italian Society of Orthopaedics and Traumatology (SIOT), Rome, Italy
(4)
Department of Orthopaedic and Traumatology, Catholic University Hospital, Rome, Italy
6.1 Gout
6.1.1 Morphological and Palaeopathological Description of the Subject
The skeleton, attributable to a senile male subject, is well built, but the bone sections have not been particularly modified by bio-mechanical stress. The horizontal cranial index suggests mesocrania (not particularly elongated shape of the skull), the frontal crests are averagely diverging, and the forehead is broad (eurymetopic). Two Wormian bones can be seen on the skull along the lambdoid suture, and some sessile exostoses are at the external auditory meatus (Fig. 6.1); these ossifications seem to be connected to a prolonged, frequent soak in cold water [1], even though many authors are inclined to think of a multifactorial aetiology [2]. As for the dento-alveolar complex, there is a large abscess cavity in correspondence with the alveoli of the first mandibular incisors (Fig. 6.2), which were lost intra–vitam; the first left molar and the second right molar are characterized, respectively, by a cavity in the tooth pulp and one in the dentine, and they both show the consequence of odontogenic abscesses on the alveolar processes. The left maxilla shows the loss of the three molars intra–vitam (the right one cannot be seen). A probable dislocation can be seen at the left temporo-mandibular joint (Fig. 6.3), with reshaping of the edge of the glenoid fossa and formation of a bone ring on the antero-superior margin of the mandibular condyle. At the insertion of the conoid and trapezoid ligaments and at the origin of the deltoid muscle on the clavicles, there are some evident enthesopatic modifications of ostheophytic nature, likely resulting from repeated shoulder movements; moreover, the enthesopathy at the insertion of the infraspinatus muscle of the right humerus confirms a frequent rotation of the humerus on the scapula. The diaphyseal index, and the enthesopathies on the interosseous tubercles of the radial bones, denotes a protruding interosseous crest, which suggest habitual forearm movements of pronation and supination; this hypothesis is also corroborated by the marked development of the attachment area of the pronator quadratus muscle of the ulnas. The flattening of the lesser trochanter, where the iliopsoas muscle is inserted, and the presence of the facet of Poirier on the femurs suggest a major flexion and abduction of the thigh; on the other hand, the enthesopathies at the origin of the tibial soleus muscle, at the insertion of the Achilles tendon and at the insertion of the plantar ligament would suggest habitual extension movements of the foot and prolonged marching on broken ground. The surfaces and the articular outline of most bone epiphyses of the appendicular skeleton are well worn, with diffused porosities and formation of bone rings. In particular, the right elbow joint is characterized by the formation of sclerotic bone plaques, at the humerus olecranon fossa and of the ulnar semilunar incisure; on the humerus condyle, an area of smooth compact bone can be seen, similar to ivory (eburnation), and the ulnar coronoid process is deformed, with expanded and jagged margins. These variations suggest diffused suffering of the joint cartilages, and their aetiology probably results from gout. The outer face of the ilium shows a new bone formation in the insertion area of the abdominal external oblique muscle (calcar crest) [3], while the attachment area of the reflexed tendon of the rectus femoris muscle is hypertrophic. A defect in the acetabulum fusion can be seen as a U-shaped notch, on the superior part of the acetabular fossa; this anomaly can be considered as a non-metric trait of almost no pathological value. As for the rachis, exuberant sindesmophytes are localized on the superior and inferior margins of the vertebral bodies; in T9-T10, the bone protuberances are linked and form a bony bridge between the two vertebrae, with a resulting ankylosis (Fig. 6.4). The fifth lumbar vertebra shows the imprint of an intraspongious hernia on the superior endplate. The costo-sternal cartilages are completely ossified, with a considerable deformity of the sternal margin.



Fig. 6.1
Auditory exostosis
Fig. 6.2
Abscess associated with first mandibular incisors
Fig. 6.3
Dislocation of the left temporo-mandibular joint
Fig. 6.4
Ankylosis of T9-T10
6.1.2 Description of the Disease
Gout is an acute inflammatory arthropathy resulting from a deposition of micro crystals. It is characterized by the deposition of monosodium urate monohydrate crystals, and this is what distinguishes it from pseudo-gout, which is characterized by the deposition of calcium pyrophosphate dihydrate. Its aetiology is often connected to a diet rich in meat and alcohol, which is the reason why it manifested in wealthy individuals. However, some other factors, such as kidney failure, can raise the plasma levels of uric acid and produce pseudo-gout signs. Males have twice as high incidence as females, while pseudo-gout is equally distributed between males and females. The clinical manifestation of gout usually follows a long period (up to a decade) of asymptomatic hyperuricemia. The typical anatomical site, almost pathognomonic, of the first gout onset is the first metacarpo-phalangeal joint, also known as podagra. The other joints, rarely the ones near the trunk such as shoulders and hips, can be affected by the following attacks. The pain of the first attack is very sharp, and resolves spontaneously, if untreated, in 5–14 days. The gout attack appears again in 90 % of cases [4]. A prolonged condition of untreated hyperuricemia or of its causes leads to tophaceous gout, with a deposition of monosodium urate monohydrate micro-crystals in the soft tissues. Gout tophi do not usually calcify, but they apply pressure on the adjacent bone structures, thus causing marginal erosion and the shape of a “mouse’s bite” on the articular bone surface (Fig. 6.5a, b). In the present case, the erosions around the head (distal meta-epiphysis) of the first metatarsus show the picture just described, and must undergo a differential diagnosis with the pseudo-pathologies (rodents’ bite) (Fig. 6.6). However, the typical site and the absence of identical lesions in other bone regions lead to an almost certain diagnosis of gout lesion on the first MT.
Fig. 6.5
Case of gout in the right (a) and left (b) medial first metatarsal
Fig. 6.6
Lateral and antero-posterior projection X-rays of the first metatarsus. The joint profile of the distal epiphysis is irregular, with higher erosion at the dorsal profile
6.1.3 Vertebra with Angioma
The patient showed an interesting additional pathological findings.

6.1.4 Radiologist’s Evaluation
Silvana Giannini,
CT Scans
Densitometric alteration with a well–defined central hypodensity and regular margins, placed in the central part of the soma with a clear hyperdensity peripheral border (Fig. 6.8). Regular densitometric representation of the adjacent bone trabeculae and absence of deformities in the opposing vertebral plates. The clear line of demarcation and the site of the lesion suggest a benign angiomatous formation, especially considering the centrifugal development typical of angiomas.
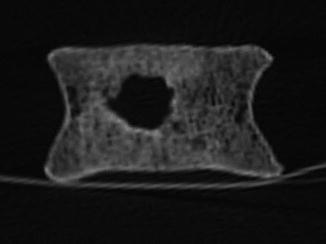
Fig. 6.8
CT scan coronal view multiplanar reconstruction: distrectual central hypodensity area with peripheral hyperdensity ring
6.2 Pott’s Disease
6.2.1 Morphological and Palaeopathological Description of the Subject
The subject, longilineal with slender upper and lower limbs, and does not seen to have undergone any severe biomechanical stress in life.
The skull is elongated (dolichocranic), with convex and not very large forehead (metriometopic).
There is a porotic hyperostosis both on the roof of the right orbit (cribra orbitalia), and on the outer table of the skull (cribra cranii). The dento-alveolar complex is compromised, in particular on the upper part, where destructive decay lesions can be seen on the first molars, three milder ones on the second premolar and on the second and third molar on the left, and a severe one on the right third molar. The alveolar process of the left first molar is affected by an odontogenic abscess. On the mandibular bone, the second and third molars are affected by mild cavities, on the buccal and occlusal surfaces, respectively.
Even though there is a medium-strong development of the muscular imprints, the enthesopathic alterations have been detected only at the origin of the triceps brachii muscle of the scapulae and at the insertion of the biceps brachii muscle of the left radius; these muscles are all involved in the forearm extension and flexion movements.
The presence of Poirier’s facets on the femoral heads and the flattening of the lesser trochanter, at the insertion of the iliopsoas muscle, both suggest flexion movements of the thigh on the pelvis, while the facets of squatting on the anterior margin of the tibio-talar joint, may have resulted from a prolonged squatting position.
The palaeopathological study has highlighted a fracture on the distal third portion of the radius and the presence of osteochondritis dissecans on the right radial capitulum (Fig. 6.9) and on the glenoid cavity of the right scapula (Fig. 6.10).


Fig. 6.9
Osteochondritis dissecans on the right radial capitulum
Fig. 6.10
Osteochondritis dissecans on the glenoid cavity of the right scapula
The fusion of the body of the sternum with the xiphoid process can be observed.
Fig. 6.11
Pott’s disease with collapse and kyphosis of the spine (a) and detail (b)
6.2.2 Description of the Disease
Spine tuberculosis is one of the oldest diseases of mankind, but although the first cases were documented in Egyptian mummies about 5,000 years ago, in modern times Sir Percival Pott described the first case of this disease in 1779 [5]. In subjects with tuberculosis (TB), the manifestation of the disease at the rachis (Pott’s disease) is rather rare (about 2 %), nevertheless it is a common site of extrapulmonary tuberculosis, accounting for about 50 % of all skeletal locations [6].
Tubercular rachis infection, compared with other infectious diseases, is connected to a greater morbidity and mortality rate, with severe complications ranging from neurological deficit to severe malformations. Risk factors for this infection are deprivation, overpopulation, malnutrition, immunodeficiency or immune suppression. The spinal location is generally secondary to the pulmonary or abdominal one, but it can also be the primary site of disease onset. The most frequent location is the short thoracic and the first lumbar segments, followed by the higher thoracic segments and by the cervical tract. The typical manifestation of the disease affects two adjacent vertebrae, less often only one vertebra, multiple vertebrae or skip-lesion (4–10 %). At first the disease affects the anterior inferior portion of the vertebral body, then it spreads to the central area of the disc. The typical sites of the disease are paradiscal, anterior, central and of the neural arch.
The central infection of the vertebral body, when the disc is not affected, spreads through the Batson venous plexus and produces a progressive shock, reaching vertebra plana. In paravertebral lesions, the disease spreads through the arteries. Young patients show a primary involvement of the disc.
The finds which are characteristic of Pott’s disease are as follows:
1.
Destruction of the inter-vertebral disc and of the adjacent vertebral bodies
2.
Collapse of the spinal elements and wedging of the anterior elements, leading to kyphosis (Fig. 6.11)
The neurological complications of Pott’s disease vary from 10 to 43 % [7]. Paraplegia is the most devastating complication. Its clinical presentation can be early or late.
The early presentation refers to a paraplegia onset during the active phases of the disease, and needs an acute treatment; its prognosis is better. The cause of paraplegia in this manifestation is the formation of pus, detritus, granulation tissue, unsteadiness due to lesion of the vertebral anterior columns, which leads to sub dislocation and dislocation.
The late presentation of paraplegia can occur after a very long period, varying from 20 to 30 years after the healing from TB active phase. It is commonly associated to a marked spinal deformity. Since bio-molecular studies are complicated and sometimes impossible on palaeopathological finds, the first line of diagnostic auxiliary tools has been the evaluation of the radiographic characteristics.
In the late stages, traditional radiography shows the typical kyphosic deformity (Fig. 6.12) of the column with several degrees, according to the collapse and wedging severity. The first signs are a reduction of the articular space, and paradiscal blurred margins of the vertebrae. In the thoracic regions, the formation of paravertebral abscesses, with necrotic tissue and granulation, is called “bird nest” and is fusiform and radio-opaque. Long lasting abscess leads to concave and excavating lesions of the anterior aspects of the vertebra, similar to aneurismatic phenomena [8].
Fig. 6.12
X-rays: lateral view shows the typical kyphosic deformity
CT scan allows a higher definition of bone alterations and their location inside the vertebral body (sclerosis, osteolysis), but also a collapsed disc and an abscess calcification inside a soft tissue. Moreover, it is useful for the definition of abscess calcifications inside the soft tissues. In vivo, it does not allow a better visualization of nervous structures than MRI, but it can be diagnostic in the analysis of skeletal findings.
The presence of calcifications inside an abscess is almost always diagnostic of spinal tuberculosis [9].
6.2.3 Radiologist’s Evaluation
Silvana Giannini
CT scans in axial, sagittal and coronal planes multiplanar reconstruction.
Metameric anterior fusion with intradiscal calcifying material, severe collapse of two vertebrae, fulcrum of the wedging (Fig. 6.13). Irregular density of the somatic limitants opposed to multiple fissures and cerebral feature with marginal erosions. In conjunction with trabecular areas of hypodensity and intrametameric ones of hyperdensity, showing the reduction to load resistance and resulting vertebral collapse. The disc spaces show hyperdense nebular precipitates, the result of phlogistic damage due to the spread of the cold abscess into the intradiscal space, which is reduced in height (Fig. 6.14). This is a valuable radiologic sign of Pott’s [10]. Anteriorly, in the site of granulomatous development, which determines the anterior vertebral collapse, small hyperdensity plates can be observed, which are remains of the calcification of the anterior longitudinal ligament. This aspect suggests an extension of the granulomatous process from the vertebral bodies and from the intradiscal area to the anterior area beneath the anterior longitudinal ligament and later in the paravertebral periosteal area [11]. The coronal level of the CT scan reconstruction shows a reduced thickness of the bone cortex with marginal encoche from modelling and some cribrate areas, compatible with excavation from organized collection. Finally, regarding the somas preserved in height, some hypodensity areas due to trabecular rarefaction can be observed, with hypodensity areas due to trabecular bundle pattern resulting from reduced osseous resistance due to altered load determined by the vertebral collapse of the metamers above.
Figs. 6.13 and 6.14
Sagittal plane multiplanar reconstruction CT scan: severe collapse of two vertebrae, fulcrum of the wedging and Metameric anterior fusion with intradiscal calcifying material
6.3 Gaucher’s Disease
6.3.1 Morphological and Palaeopathological Description of the Subject
The skeleton, pertaining to an adult male subject, shows a high skull (hypsicranic), with very diverging frontal crests, large orbits (hypsiconchic) and a long and narrow nose (leptorrhine); the cranial index denotes mesocrany. Small bony formations (4 and 5 mm) can be observed on the anterior edge of the foramen magnum, at the basion. A pair of button osteomas can be seen on the outer table of the right emi-frontal bone; moreover, a widespread porotic hyperostosis can be observed on the cranial theca (cribra cranii) (Fig. 6.15) and on the roof of the orbits (cribra orbitalia). The ante–mortem loss of some dental elements can be observed both on the maxillary and the jaw bones, in particular, the alveolar processes of the superior left first molar and inferior second premolars and first molars are completely resorpted.

Fig. 6.15
Cribra cranii
The subject is robust, but both upper and lower limbs sections are not particularly modified by biomechanical stress.
The upper right limb is longer than its contra-lateral, even though the differences in size do not apply the other parameters: as a matter of fact, there are no meaningful differences either between the transverse diameters, or between the circumferences and the muscular insertions are more marked on the left. A biomechanical stress of the pectoralis major muscle on the humerus and of the deltoid muscle is detected, both at the clavicular origin and at the humeral insertion. Repeated adduction and abduction movements of the arm may have lead to the detected lesions. The lower limbs show some enthesopathies at the insertion of the vastus medialis and soleus muscles, which may suggest repeated extension movements of the leg on the thigh and of the foot. The axial skeleton is the area which is most frequently affected by degenerative phenomena, above all in the dorsal portion of the rachis; signs of discal distress, in the shape of wide and deep intraspongious hernias (Fig. 6.16), can be observed on the vertebral bodies of the thoracic and lumbar tracts; superiorly L3 and L4 show two oval depressions affecting the posterior right quadrant of the disc and in both cases cross the annulus imprint. A widespread presence of Schmörl hernias suggests intense and prolonged compression on the vertebral axis. The appendicular skeleton shows mild degenerative phenomena that can only be seen at the level of the acetabular fossae of the coxal bones and of the superior margin of the first sacral vertebra. Small articular lesions, with a local detachment of the cartilage and local subchondral bone necrosis (osteochondritis dissecans), can be observed on the lateral condyles of both femurs and on the distal articular surface of the right tibia. Three right ribs show macroscopic signs of previous fractures, with the complete ossification of the bone callus.










