Chapter 6 Impairment Rating and Disability Determination
This chapter includes a brief introduction to the latest (sixth) edition to the American Medical Association (AMA) Guides to the Evaluation of Permanent Impairment,48 a reference text that can be likened to an updated tax code for impairment rating. The sixth edition chief editor is Robert D. Rondinelli, a physiatrist. In contrast to previous editions of the AMA Guides, it is fortunate that the sixth edition moves toward a more functional view of impairment rating.
This chapter is not intended to be used to determine impairment or disability for a specific patient. The reader is referred in this regard to the AMA Guides,48 which outlines a method for rating impairment for virtually every organ system. In practical terms, however, most impairment and disability evaluations focus on musculoskeletal disorders.
Disability Agencies
The VA has its own disability benefits program, described as follows:
Disability compensation is a monetary benefit paid to veterans who are disabled by an injury or disease that was incurred or aggravated during active military service. These disabilities are considered to be service-connected. Disability compensation varies with the degree of disability and the number of veteran’s dependents, and is paid monthly.60
Definitions: Disability and Impairment
Social Security Administration
Agencies have different definitions of disability. For example, the SSA defines disability as “the inability to engage in any substantial gainful activity … by reason of any medically determinable physical or mental impairment that can be expected to result in death or that has lasted or can be expected to last for a continuous period of not less than 12 months.”56 To determine work disability, the SSA uses a sequential evaluation process that focuses on applicants’ diagnoses, not their functional abilities. Although the SSA’s five-step process assesses earnings and impairment severity, it is not until late in the process that functional capacity is assessed. An applicant may appeal an unfavorable disability determination, which can markedly extend processing time. Unlike the VA, the SSA does not award benefits for “partial disability.”
AMA Guides, Sixth Edition
The latest edition of the AMA Guides48 uses as its foundation the World Health Organization model of disablement. This model is called the International Classification of Functioning, Disability, and Health (ICF) and is illustrated in Figure 6-1. There are three key inputs to the ICF model determining disability, paraphrased here from the AMA Guides48:
Note that body functions are physiologic—for example, the ability of the upper limb to generate accurate motion and strength. Body structures are anatomic—for example, the upper limb itself. Either or both can be compromised to produce impairment. The inability to carry out tasks, such as not being able to comb one’s hair, is an activity limitation. The inability to be involved in a typical life situation, such as being gainfully employed and interacting with one’s peers, is a participation restriction. Note that there is not a necessary correlation between activity limitation and participation restriction.
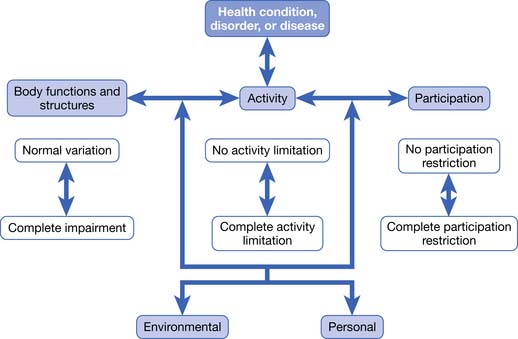
FIGURE 6-1 The World Health Organization ICF Model of Disablement.
(Redrawn from Rondinelli RD, editor: Guides to the evaluation of permanent impairment, ed 6, Chicago, 2008, American Medical Association Press.)
In the ICF model, there is no linear progression from pathology to impairment to disability and to participation restriction. The AMA Guides justifies the use of the ICF model as follows48:
Impairment rating within the latest AMA Guides10 has more weight given to loss of function in the determination of impairment rating. This is defined as a “consensus-derived percentage estimate of loss of activity reflecting severity for a given health condition, and degree of associated limitations in terms of ADLs [italics added].”
This chapter is not meant to provide the reader with the necessary skills to do actual impairment ratings, which can be fairly complex and detailed. However, a brief sketch of the approach to impairment rating based on the latest AMA Guides is given here48:
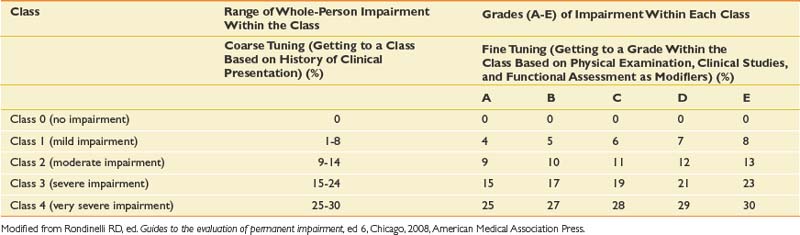
Note that there is a new emphasis on functional history with this edition of the AMA Guides. Loss of function is assessed in part by self-report measures that claimants may fill out at the time of their impairment evaluations. Different measures are used for different kinds of disorders; for example, the QuickDASH is used for disorders of the hand, while the Pain Disability Questionnaire is used for evaluating functional limitations involving the spine. The important general point is that impairment ratings in the AMA Guides sixth edition incorporate subjective information from claimants about their burden of illness. The significance of this change in the Guides is modest, however, because functional history plays a relatively minor role, modulating the grade within a given class. The primary emphasis in the Guides continues to be on objective findings rather than subjective history in the impairment rating process.
Further Thoughts on Impairment Versus Disability
Roles of Physicians in Disability Evaluation
Many physicians do not seek opportunities to perform disability evaluations because they are uncomfortable evaluating disability in patients whom they are treating. They correctly perceive that the process of disability evaluation places a physician between the interests of the patient and those of an insurance company or disability agency. In the best of circumstances, this can seem to the physician like trying to fit a round peg into a square hole, because the categories of disability established by such agencies often do not match the clinical realities of patients.
The concerns that treating physicians have about doing disability evaluations appear to fall into two categories: knowledge deficits and ethical concerns. Physicians who work primarily as clinicians are likely to be unfamiliar with the disability laws and regulations relevant to their patients, and the disability agencies that administer them. They are also likely to lack expertise in the mechanics of rating impairment, such as those detailed in the AMA Guides,48 and in the methods that can be used to assess work ability.20,21,31,33,49
Treating physicians can be concerned about conflicts between the clinical role they normally play when they treat patients and the adjudicative role that is required during a disability evaluation. Informal observation as well as examination of the limited literature on these roles26,42,58,65 suggests several differences between the two roles. For example, physicians performing disability evaluations are expected to focus on objective findings and legal responsibility, including causation, for an examinee’s disorder, but these are not the main concern of physicians when they provide clinical treatment.46 As Sullivan and Loeser58 have noted, significant ethical issues arise when physicians switch back and forth between these two roles.
Assessing Self-Reports of Patients Regarding Physical Capacity
A key challenge is to combine examinees’ self-reports regarding their incapacitation with objective medical information relevant to their injury.47 Note that the definition of “objective medical information” is not always clear. Unfortunately the existence of objective medical findings often depends on the degree to which technologies have advanced. For example, before myelography became available, radiographic studies (i.e., x-ray films) did not demonstrate objective findings for patients with radiculopathies.
A position somewhere between these two extremes is probably most appropriate. The perceptions that patients have about their abilities certainly should not be ignored or discounted. As a practical matter, research demonstrates that these self-appraisals are important predictors of whether patients with pain problems will perform well on physical tests or will succeed in terminating their disability, or both.14,15,23–25,30 Physicians who make disability decisions without considering patients’ appraisals are discarding valuable data. As a result, their decisions can go awry in two ways. First, they can pressure patients to return to work in jobs that the patients are realistically not capable of performing. Second, they can be ineffective in resolving disability issues. Consider patients who are released to work by their treating physician or by an independent medical examiner even though they are convinced that they are unable to work. Such patients are likely to retain an attorney and start a protracted legal battle regarding their work status.
But the fact that patients’ perceptions are important does not mean that they are valid or immutable. In fact, research on patients with disability related to chronic pain suggests the opposite: some often have distorted views of their capabilities, and these views are modifiable.1,12,28,35 Disability evaluators need to consider the validity of a patient’s stated activity limitations in light of the biomedical information available and their assessment of the patient’s credibility. Evaluators should reserve the right to challenge the patient’s self-assessments and to make decisions that are discordant with these assessments.
Blending Administrative Imperatives With Patient Realities






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


