Chapter 16 Spinal Orthoses
History of Spinal Orthotic Management
The first evidence of the use of spinal orthoses can be traced back to Galen (c.131 to 201 AD). Primitive orthotic devices were made of items that were readily available during this period (Figure 16-1). These items consisted of leather, whalebone, and tree bark. Spinal orthoses, although crude in their construction, have been recovered by archaeologists from the cliff dwellings of pre-Columbian Indians. The word orthosis is Greek and means “to make straight.”2 Ambroise Paré (1510 to 1590) wrote about bracing and spinal supports, and Nicholas Andry (1658 to 1742) coined the term orthopaedia, pertaining to the straightening of children.4 Unstable areas such as fractures were often held in a corrected position with an orthosis, to allow for healing to occur. Normally fixed deformities were accommodated while flexible deformities were corrected. Orthopaedia was the predecessor to the field of orthotics.1

The primary goal of modern orthoses is to aid a weakened muscle group or correct a deformed body part. The orthosis can protect a body part to prevent further injury, or can correct the position (immediate term or long-term) of the body part. The same approach is true for spinal orthoses. The clinician’s priority should be to determine which spinal motion to control. Good clinical outcomes can be maximized through the proper selection, use, and application of the orthosis. (See Chapters 14 and 15 for further information on orthoses.)
Terminology
Prefabricated Versus Custom Orthoses
The availability of prefabricated orthoses today presents the rehabilitation team with a variety of choices and some challenges. Many of the prefabricated orthoses come in various sizes and can be fitted to patients often with little or no adjustment. While this can be a benefit to the patient and the team in terms of time, care should be taken to ensure that the design and function of these orthoses are appropriate for the patient’s condition and not used purely for convenience. Custom orthoses, in most cases, provide a more comfortable fit with a higher degree of control, and can be designed to accommodate a patient’s unique body shape or deformities. Recognition of the time needed to fabricate the orthosis, the experience of the fabricator, the patient’s specific condition, and the expectations of the patient are all factors that should be considered when ordering a custom orthosis.
Spinal Anatomy
The vertebral column is composed of 33 vertebrae, including 7 cervical, 12 thoracic, 5 lumbar, 5 inferiorly fused vertebrae that form the sacrum, and 5 coccygeal. The spinal column not only bears the weight of the body, but it also allows motion between body parts and serves to protect the spinal cord from injury. Before birth, there is a single C-shaped concave curve anteriorly. At birth, infants have only a small angle at the lumbosacral junction. As a child learns to stand and walk, lordotic curves develop in the cervical and lumbar region (age 2 years). These changes can be attributed to the increase in weight-bearing and differences in the depth of the anterior and posterior regions of the vertebrae and disks.28,32
The spine is composed of more than vertebral bodies. The intervertebral disk is composed of a nucleus pulposus, annulus fibrosus, and cartilaginous end plate. Disks make up approximately one third of the entire height of the vertebral column. The nucleus contains a matrix of collagen fibers, mucoprotein, and mucopolysaccharides. They have hydrophilic properties, with a very high water content (90%) that decreases with age.27 The nucleus is centrally located in the cervical thoracic spine, but more posteriorly located in the lumbar spine. The annulus fibrosus has bands of fibrous laminated tissue in concentric directions, and the vertebral end plate is composed of hyaline cartilage.
Normal Spine Biomechanics
Movement of the vertebral column occurs as a combination of small movements between vertebrae. The mobility occurs between the cartilaginous joints at the vertebral bodies and between the articular facets on the vertebral arches. Range of motion is determined by muscle location, tendon insertion, ligamentous limitations, and bony prominences. In the cervical region, axial rotation occurs at the specialized atlantoaxial joint. At the lower cervical levels, flexion, extension, and lateral flexion occur freely. In these areas, however, the articular processes, which face anteriorly or posteriorly, limit rotation. In the thoracic region, movement in all planes is possible, although to a lesser degree. In the lumbar region, flexion, extension, and lateral flexion occur, but rotation is limited because of the inwardly facing articular facets.11 An understanding of the three-column concept of spine stability/instability is helpful to ensure that the proper orthosis is prescribed. The anterior column consists of the anterior longitudinal ligament, annulus fibrosus, and the anterior half of the vertebral body. The middle column consists of the posterior longitudinal ligament, annulus fibrosus and the posterior half of the vertebral body. The posterior column consists of the interspinous and supraspinous ligaments, the facet joints, lamina, pedicles, and the spinous processes. The loss of normal spinal anatomy can affect the stability of the spine.
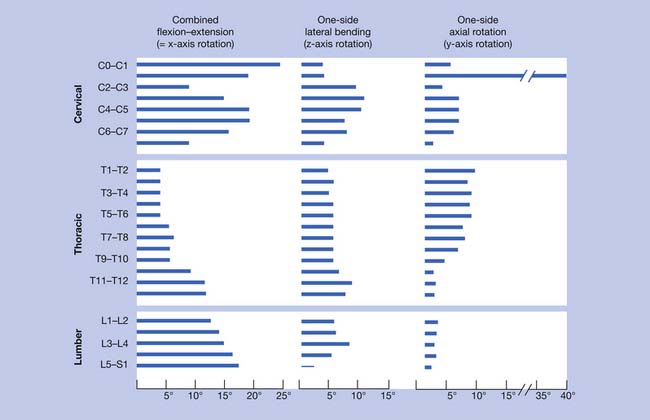
Spine motion can be classified with reference to the horizontal, frontal, and sagittal planes. Spinal motion can shift the center of gravity, which is normally located approximately 2 to 3 cm anterior to the S1 vertebral body. White and Panjabi33 provided a summary of the current literature, revealing motion in flexion and extension, laterally, and axially (Figure 16-2). In the cervical spine, extension occurs predominantly at the occipital C1 junction. Lateral bending occurs mainly at the C3–C4 and C4–C5 levels. Axial rotation occurs mostly at the C1–C2 levels. In the thoracic spine, flexion and extension occur primarily at the T11–T12 and T12–L1 levels. Lateral bending is fairly evenly distributed throughout the thoracic levels. Axial rotation occurs mostly at the T1–T2 level, with a gradual decrease toward the lumbar spine. The thoracic spine is the least mobile because of the restrictive nature of the rib cage. In the lumbar spinal segment, movement in the sagittal plane occurs more at the distal segment, with lateral bending predominantly at the L3–L4 level. There is insignificant axial rotation in the lumbar spinal segment.
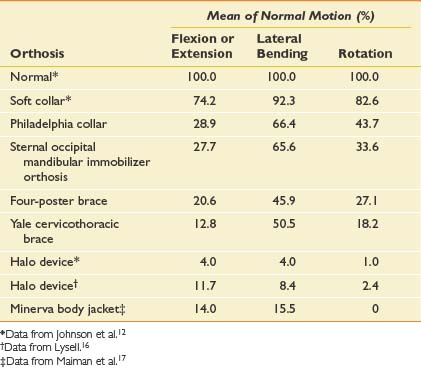
Knowledge of the normal spinal range of motion helps in understanding how the various cervical orthoses can limit that range (Table 16-1). Soft collars provide very little restriction in any plane. The Philadelphia-type collar mostly limits flexion and extension. The four-poster brace and Yale orthosis have better restriction, especially with flexion-extension and rotation. The halo brace and Minerva body jacket have the most restriction in all planes of motion.
Table 16-1 Normal Cervical Motion From Occiput to First Thoracic Vertebra and the Effects of Cervical Orthoses
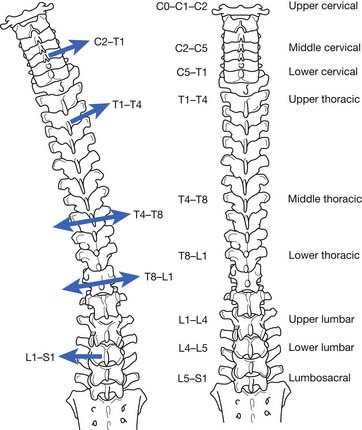
An interesting phenomenon related to movement in the spine occurs during motion. If the movement along one axis is consistently associated with movement around another axis, coupling is occurring. For example, if a patient performs left lateral movement (frontal plane) motion, the middle and lower cervical and upper thoracic spine rotate to the left in the axial plane (Figure 16-3). This causes the spinous processes (posterior side of the body) to move to the right. In the lower thoracic spinal segment, left lateral movement in the frontal plane can cause rotation in the axial plane, with the spinal processes moving in either direction. The lumbar area has a contradictory movement pattern when compared with the cervical spine. With left lateral bending of the lumbar spine, the spinous processes move to the left. A three-dimensional perspective is important to maintain during examination. Patients with scoliosis and patients who undergo radiologic testing would benefit from an evaluation for the normal coupling patterns noted.
Nachemson21–23 performed the classic studies on normal adults that measured intradiskal pressures during a variety of activities and positions. Standing pressure was referenced as 100 in the lumbar disk. Lowest pressure measurements were noted in the supine position, with progressively higher pressures in the following positions: side lying, standing, sitting, standing with hip flexion, sitting with forward flexion, standing with forward flexion, and lifting a load while sitting with forward flexion.24
Description of Orthoses
Head Cervicothoracic Orthoses
Type: Halo Orthosis
Biomechanics
The halo orthosis (Figure 16-4) provides flexion, extension, and rotational control of the cervical region. Pressure systems are used for control of motion, as well as to provide slight distraction for immobilization of the cervical spine.

Design and Fabrication
This orthosis provides maximum restriction in motion of all the cervical orthoses. It is the most stable orthosis, especially in the superior cervical spine segment. A halo is used for approximately 3 months (10 to 12 weeks) to ensure healing of a fracture or of a spinal fusion. Usually a cervical collar is indicated after the halo is removed, because the muscles and ligaments supporting the head become weak after disuse. All pins on the halo ring should be checked to ensure tightness 24 to 48 hours after application, and retorqued if necessary.
Cervical Orthoses
Type: Philadelphia or Miami J
Biomechanics
The Philadelphia (Figure 16-5) and Miami J (Figure 16-6) orthoses provide some control of flexion, extension, and lateral bending, and minimal rotational control of the cervical region. Pressure systems are used for control of motion, as well as to provide slight distraction for immobilization of the cervical spine. Circumferential pressure is also intended to provide warmth and as a kinesthetic reminder for the patient.

< div class='tao-gold-member'>


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


