Chapter 2 Examination of the Pediatric Patient
Assessment of an infant or a child requires that the examiner has the ability to attain a complete medical, developmental, and family history; has a flexible approach to the physical examination; and understands the unique interaction between a child and that child’s physical and psychosocial environment. Establishing a diagnostic label is important, but determining the child’s functional status is also important for the rehabilitation management of the child. Although the evaluation of children has many similarities to that of adults (see Chapter 1), it also has many distinctive features, as highlighted in this chapter.
Diagnostic Evaluations
History
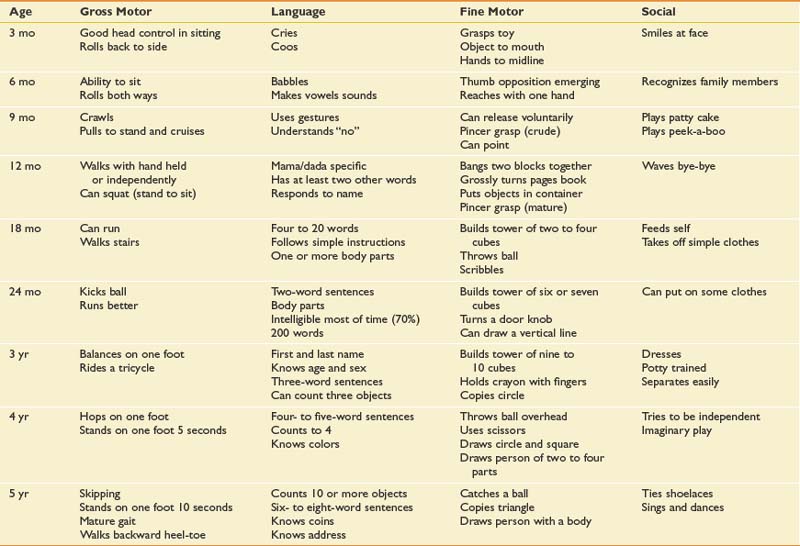
A history should include a determination of the ages at which major developmental milestones were met, because this aids in assessing deviations from normal (Table 2-1). The achievement of major landmarks in gross motor, fine motor, and adaptive skills; in speech and language; and in personal and social behavior should clarify whether the disability is confined primarily to the neuromuscular system or involves deficits in other areas as well. The coexistence of multiple problems influences the rehabilitation program, interventional methods, and ultimate outcome.
A family history can assist in the identification of inherited or congenital diseases. A query of multigenerational medical problems should be obtained and formal genetic counseling offered if an inherited disease is suspected or known to exist. It is frequently helpful to briefly examine a family member if a genetic disorder is suspected. For example, assessing a parent for grip myotonia or the inability to release and quickly open up the hand can be done with a simple handshake. Examination of the parent’s foot can demonstrate a pes cavus or high-arched foot, which when present in the child is suggestive of the autosomal dominant form of Charcot-Marie-Tooth disease (see Chapter 47).
Physical Examination
There is no standardized approach to the physical examination of infants and children.1,5,21,22,29 Pediatric examinations are tailored to the individual child, based on age and developmental stage. Knowledge of developmental stages is important in evaluating both acute and chronic diseases. Young children should be examined with the parents present, but the parents’ presence is optional for adolescents.
Growth
Growth during infancy occurs at a very rapid rate, slows during early childhood, and increases once again during adolescence. Routine health care visits should emphasize the evaluation of growth parameters for every child, including height, weight, and head circumference. It is critical for a child’s growth to be plotted on age- and gender-appropriate charts.9 Growth is influenced not only by genetic programming but also by medical conditions and nutrition. The onset of organic or psychosocial illness might be accompanied by a sudden acceleration or cessation of growth. The rate of growth is more important than the absolute values, as evidenced by a child whose head circumference increases from the 5th percentile to the 50th percentile in a 2-month period, representing untreated hydrocephalus. Growth charts are now available for specific genetic syndromes, including Turner and Down syndromes, and for specific disabilities such as quadriplegic cerebral palsy.
Head circumference is measured serially using the occipitofrontal circumference. The average head circumference at birth is 35 cm and increases to 47 cm by 1 year of age.25 Microcephaly is defined as a head circumference that falls below two standard deviations from the mean, and is suggestive of central nervous system abnormalities including congenital infections, anoxic encephalopathy, or a degenerative disorder. Macrocephaly, defined as a head circumference greater than two standard deviations above the mean, can be associated with hydrocephalus, a metabolic disease, or the presence of a mass and requires further evaluation. Approximately 50% of macrocephaly in children is familial. Parental head size should be plotted on adult growth charts. A child with an isolated large head, no developmental delays, and a parent with a large head is probably normal.
The average height of a newborn is 50 cm, increasing by 50% at 1 year of age and doubling by 4 years.25 An estimate of adult height is obtained by doubling the child’s height at age 2 years. Many genetic syndromes are associated with short stature, including Down and Turner syndromes. Birth weight is influenced by multiple parameters and includes parental size, nutrition, gender, genetics, gestation and health of the baby. The average full-term child in the United States has a birth weight of 3400 g. Birth weight should double by 5 months of age and triple by 1 year of age. Deviations from normal weight should alert the provider to potential health-related problems that need to be investigated.
Adolescents pass through a predictable sequence of pubertal events as they mature. The Tanner stages of sexual maturity describe the secondary sexual characteristics of teenage girls and boys.33,34 Assessment of breast development and pubic hair in girls, and genital size and pubic hair in boys, is the basis for assigning a Tanner stage to an adolescent. The average age of menarche in girls is typically around 12 years. Precocious puberty is diagnosed if there is a premature development of secondary sexual characteristics. It is present when there are findings of puberty in girls younger than 8 years and in boys younger than 9 years.55 The etiology can be either peripheral or within the central nervous system, such as a hypothalamic-pituitary abnormality. Precocious puberty is well documented in children with spina bifida and brain injuries.51 Tanner staging is useful in evaluating musculoskeletal issues such as leg length discrepancies and scoliosis, as treatment options can vary depending on the pubertal stage of the child.
General Inspection
Visual inspection is critical in the examination of a child. It begins with a general assessment of the child’s appearance. This gives the examiner a sense of how the infant or child interacts with the parents as well as information about the child’s general movements, abnormal physical features, and overall general health. The presence of abnormal physical features can be helpful in identifying common syndromes (Table 2-2). The examiner should pay specific attention to facial abnormalities such as abnormal spacing of the eyes, position and size of the ears and philtrum, and size of the upper and lower jaws. Normal measurements can be referenced when attempting to distinguish specific features such as ocular hypertelorism or small-appearing ears.26
Table 2-2 Common Syndromes and the Associated Abnormal Features
| Syndrome | Abnormalities |
|---|---|
| Angelman syndrome | Severe mental retardation, delay in attainment of motor milestones, microbrachycephaly, maxillary hypoplasia, deep-set eyes, blond hair (65%), ataxia and jerky arm movements resembling those of a marionette (100%), seizures |
| Hunter syndrome | Growth deficiency, coarsening of facial features, full lips, macrocephaly, macroglossia, contractures of joints, broadening of bones, hepatosplenomegaly, delayed tooth eruption |
| Marfan syndrome | Tall stature with long slim limbs, little subcutaneous fat, arachnodactyly, joint laxity, scoliosis (60%), retinal detachment, upward lens subluxation, dilatation of ascending aorta |
| Neurofibromatosis syndrome | Areas of hyperpigmentation or hypopigmentation with café au lait spots (94%); “freckling” of axilla, inguinal folds, and perineum; cutaneous neurofibromas that are small, soft, pigmented nodules; plexiform neurofibromas; Lisch nodules |
The assessment of the head and neck includes inspection of shape and symmetry. Since the American Academy of Pediatrics initiated the Back to Sleep program in 1992, the recommendation for newborns and infants to sleep in the supine position, more infants are presenting to their primary care providers with the presence of plagiocephaly, primarily observed as a unilateral flattening of the occiput.41 Examination of the head and neck can also identify the presence of torticollis involving tightness of the sternocleidomastoid muscle. Children with torticollis have a head tilt to the involved side, and the chin will be turned to the contralateral side. Children with a short, broad neck with webbing might have Klippel-Feil syndrome, and with girls Turner syndrome must be considered.
Musculoskeletal Assessment
The spine and back examination includes an assessment of the bones and muscular elements, as well as a postural assessment. Evaluation includes having the child stand or sit while the back is examined. The height of the shoulders, position of scapula, and height of the pelvis should be assessed. The child is asked to bend forward so the examiner can look for rib and back asymmetries indicating scoliosis (Figure 2-1). Radiographs of the spine help define the severity of kyphotic and scoliotic curves. Scoliosis is categorized as infantile, juvenile, adolescent, or neuromuscular. The most common form is adolescent idiopathic scoliosis seen in pubertal girls with a right thoracic curve.35 Children should also be evaluated for other spinal pathology (Table 2-3).
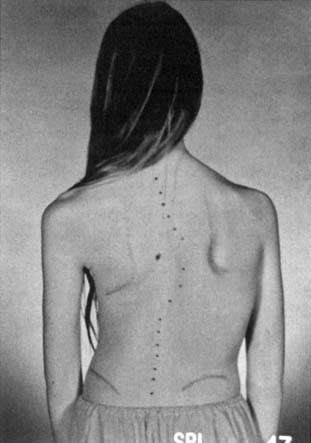
Table 2-3 Spinal Abnormalities
| Spine Abnormality | Clinical Findings |
|---|---|
| Scoliosis (idiopathic, congenital, neuromuscular) | |
| Kyphosis (congenital, Scheuermann, neuromuscular) | Abnormal posture increases with flexion |
| Spondylolisthesis |
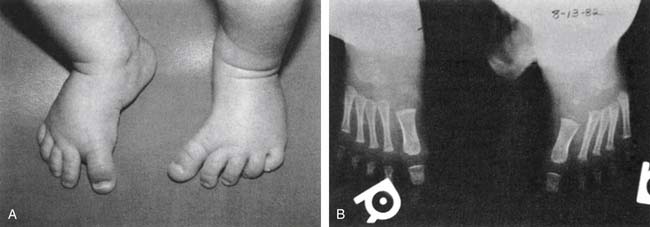
Examination of the lower limbs includes an evaluation of joint range of motion and torsional forces. Most torsional deformities tend to correct spontaneously as children grow and develop. Evaluation of the foot includes the toes and the three parts of the foot: forefoot, midfoot, and hindfoot. The shoes should be assessed for patterns of wear. The most common foot deformity is metatarsus adductus, which is medial deviation of the metatarsal bones (Figure 2-2). It is usually caused by intrauterine position, and the severity of the deformity can be classified according to the flexibility of the foot. Mild anomalies are easily corrected, while moderate cases require that some force be applied to the foot. Severe abnormalities cannot be corrected by conservative means and should be referred to an orthopedic surgeon.
Pes planus, or flatfoot, is a normal variant seen in children up to the age of 3 to 5 years.49 It occurs when the medial longitudinal arch is not well developed or there is underlying ligamentous laxity. Flexible flatfeet can also be a normal variant into adulthood, as long as an arch forms when individuals stand on their toes. Rigid or painful feet with reduced subtalar joint motion are often associated with tarsal coalition. This is an abnormal fusion of two or more bones in the midfoot or hindfoot that restricts motion. The two most common joints involved are the talocalcaneal and calcaneonavicular. Congenital vertical talus is a rigid flatfoot deformity with a rocker bottom and a dorsal dislocation of the navicular on the talus. It is associated with the genetic syndromes of myelodysplasia and arthrogryposis.
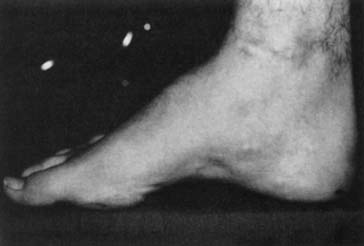
Pes cavus is a high-arched foot that does not flatten with weight-bearing. It is often associated with clawing of the toes, hindfoot varus, plantar fascia contractures, and great toe cock-up deformities. It can be a normal variant or might indicate a neuromuscular disorder such as Charcot-Marie-Tooth disease (Figure 2-3).
Congenital talipes equinovarus, or the classic clubfoot, is a complex deformity characterized by a small foot with a medial border crease, hindfoot equinus, and forefoot and hindfoot varus, along with forefoot adductus.43 The etiology remains controversial, as several theories have been proposed, including intrauterine position, primary germ cell defect in the talus causing persistent plantar flexion and inversion, and soft tissue abnormalities affecting the neuromuscular units. There is an association with other disorders such as cerebral palsy, arthrogryposis, chromosomal abnormalities, spina bifida, and neuromuscular diseases.
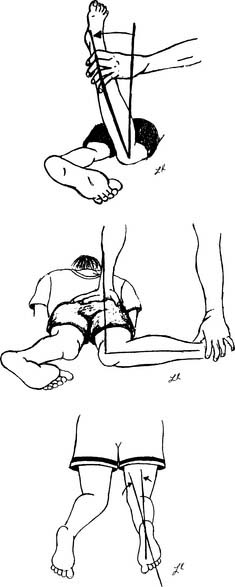
Tibial torsion is a twisting of the distal tibia in relationship to the proximal segment.32 It can result in either internal or external rotation of the tibia and can cause an abnormal-appearing gait pattern. Children have approximately 5 degrees of internal tibial torsion at birth, which progresses to 10 to 15 degrees in the adult. It is the most common reason for intoeing in the toddler age range. The evaluation includes assessment of the position of the patella during gait, along with the thigh-foot angle (Figure 2-4). Thigh-foot angle is assessed in the prone position with the knee flexed to 90 degrees. Two bisecting lines are drawn: one along the femur and the other through the heel and third web space. The angle should be −10 degrees to +10 degrees.
< div class='tao-gold-member'>
Related posts:
 Psychological Assessment and Intervention in Rehabilitation
Employment of Persons with Disabilities
Transplantation of Organs: Rehabilitation to Maximize Outcomes
Electrodiagnostic Medicine II: Clinical Evaluation and Findings
Manipulation, Traction, and Massage
Musculoskeletal Disorders of the Upper Limb
Psychological Assessment and Intervention in Rehabilitation
Employment of Persons with Disabilities
Transplantation of Organs: Rehabilitation to Maximize Outcomes
Electrodiagnostic Medicine II: Clinical Evaluation and Findings
Manipulation, Traction, and Massage
Musculoskeletal Disorders of the Upper Limb
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


