Chapter 5 Gait Analysis
Technology and Clinical Applications
Since the later part of the twentieth century, gait analysis has become a useful clinical tool in the management of walking and movement problems for patients with neurologic and orthopedic conditions. Technology related to gait analysis and our understanding of the role of gait analysis in clinical assessment and management have improved significantly in recent years. Gait analysis was initially used in the last decade of the nineteenth century by the Weber brothers. Muybridge21 contributed to the understanding of movement with his famous sequential photographs, first of horses and later of walking and running men. Composited animations of some of Muybridge’s original work can be seen online (http://photo.ucr.edu/photographers/muybridge/contents.html). Later, Marey19 used light-colored marking strips on dark-clad subjects for the analysis of body movements. Bernstein2 initiated the formal study of kinematics with his detailed photographic studies of normal human locomotion movement. In 1947 Schwartz et al.24 made the first quantitative studies of the forces generated at the floor-foot interface during walking. Later, electromyography (EMG) recordings were possible. Inman’s group13 at the University of California Biomechanics Laboratory refined the simultaneous recording of multiple muscle group activity during normal ambulation.
Gait analysis has evolved into a recognized objective medical evaluation technique that is important in surgical planning10 and in the planning of other therapeutic interventions, such as botulinum toxin injection in the management of spasticity and the prescription and optimization of lower extremity orthotic and prosthetic devices.8 Other applications include sport movement analysis, analysis of other musculoskeletal conditions, and outcomes measurement. The most important contribution of gait analysis might be as a quantitative assessment tool for movement generally and walking specifically. In some centers, computer models of walking are used to drive simulation models that are then modified with the proposed interventions to determine whether the treatment will achieve the desired goal.
These criteria require that the clinician be familiar with the complex physiologic interactions of normal gait biomechanics, with normal and abnormal patterns of motor control, and with the technology used for its assessment. In addition, the clinician must possess the ability to relate these features to the pathologic motion that is observed during walking to effectively diagnose and address the problems of abnormal gait. To properly identify and evaluate the gait problems of the patient, the clinician must be able to produce a hypothesis and then attempt to understand what the problem is, where and when it is present, and why it occurs. Knowledge of appropriate available interventions, as well as a thorough medical history and examination, is needed to determine the most appropriate treatment interventions.7
Normal Locomotion
Walking requires significant motor coordination, yet most people can perform this complicated task without even thinking about it. The fundamental objective of bipedal human locomotion is to move safely and efficiently from one point to another.3 Humans are the only animals who characteristically have upright walking. Gait can be described as an interplay between the two lower limbs, one in touch with the ground, producing sequential restraint and propulsion, while the other swings freely and carries with it the forward momentum of the body. Most healthy individuals accomplish walking in a similar manner between the ages of 4 and 8 years because everyone has the same basic anatomic and physiologic makeup. Gait patterns are highly repeatable both within a subject and between subjects, but clearly each person has a unique walking style.
Gait is cyclic and can be characterized by the timing of foot contact with the ground; an entire sequence of functions by one limb is identified as a gait cycle (Figure 5-1).3,13 Each gait cycle has two basic components: stance phase, which designates the duration of foot contact with the ground, and swing phase, the period during which the foot is in the air for the purpose of limb advancement. The swing phase can be further divided into three functional subphases: initial swing, midswing, and terminal swing. In the same manner the stance phase can be partitioned into one event and four subphases: initial contact, loading response, midstance, terminal stance, and preswing.1,6
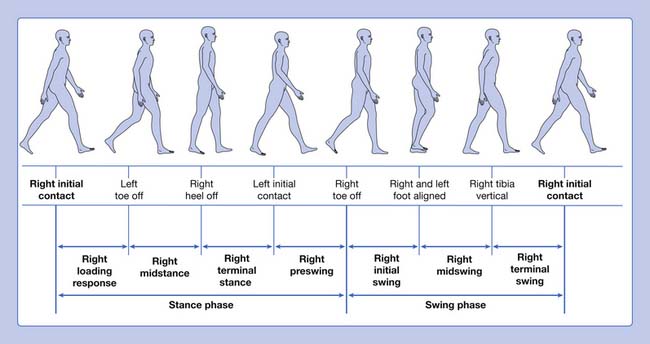
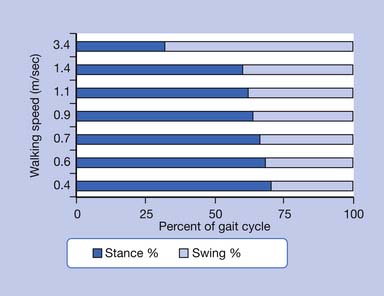
The stance phase can alternatively be subdivided into three periods according to foot-floor contact patterns. The beginning and the end of the stance phase mark the period of double support, during which both feet are in contact with the floor, allowing the weight of the body to be transferred from one limb to the other. When double support is absent, the motion is, by one definition, running. Single limb support begins when the opposite foot is lifted from the ground for the swing phase. For normal subjects walking at self-selected comfortable speeds, the normal distribution of the floor contact period during the gait cycle is broadly divided into 60% for the stance phase and 40% for the swing phase, with approximately 10% overlap for each double support time. These ratios vary greatly with changes in walking velocity (Figure 5-2).
The step period is the time measured from an event in one foot to the subsequent occurrence of the same event in the other foot. There are two steps in each stride or gait cycle. The step period is useful for identifying and measuring asymmetry between the two sides of the body in pathologic conditions. Step length is the distance between the feet in the direction of progression during one step. The stride period is defined as the time from an event of one foot until the recurrence of the same event for the same foot; initial contact to initial contact is used to define the stride period. Stride length is the distance between the same foot in the direction of progression during one stride. Left and right strides are equal in normal ambulation, but this might not be the case in pathology. The stride period is often time-normalized for the purpose of averaging gait parameters over several strides both between and within subjects (i.e., the absolute time is transformed to 100%). Cadence refers to the number of steps in a period of time (commonly expressed as steps per minute). The step length, step time, and cadence are fairly symmetric for both legs in normal individuals. These are all useful parameters when evaluating pathologic gait. The base of support refers to the lateral distance between the feet. This is usually measured as the perpendicular distance between the medial borders or centerlines of the left and right feet.
Gait Dysfunction
Because of the complex relationship of multiple body segments, it is difficult to clearly identify the primary cause and compensation (substitution) in a gait deviation. One approach is to look at the different phases of locomotion and identify factors that affect the particular expected functional component when attempting to understand pathologic gait. Following this functional approach, the stance phase dysfunctions can be categorized into three groups, as shown in Box 5-1.
Ankle-Foot Instability
The foot interaction with the ground is inadequate, interfering with its inherent weight-bearing function. This can be exemplified as an abnormal posture of the foot present in the form of equinus, equinovarus, ankle valgus with or without equinus, toe flexion, hallux extension (hitchhiker’s great toe),20 and/or excessive ankle dorsiflexion as seen with insufficient plantar flexor strength. Ankle-foot instability problems are commonly seen in the patient with neurologic sequelae after central nervous system injuries.
Quantitative Gait Analysis
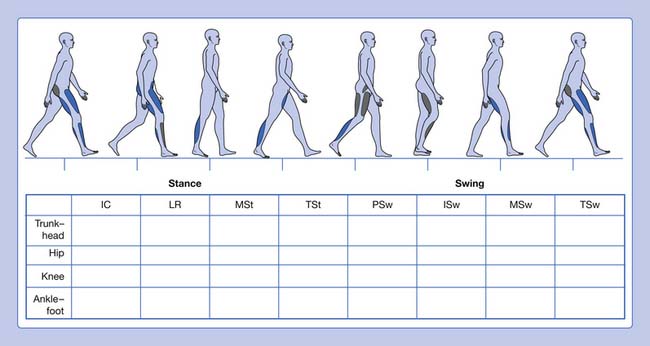
Informal visual analysis of gait is routinely performed by clinicians and used as the basis to develop the initial questioning and examination of a patient (Table 5-1). This sometimes casual observation can be more useful, albeit with many limitations, if performed in a careful, systematic manner. This can be done using a simple form that guides the clinician on documenting the findings (Figure 5-3). This type of analysis can yield good descriptive information, especially when slow-motion video technology is used to supplement it. The complexity and speed of events that occur during walking, coupled with deviations and possible compensations that occur in pathologic gait, define the limitations of a visual-based qualitative analysis of locomotion.3 Fortunately there are a great many tools available to increase our ability to observe and quantify gait.
Table 5-1 Phases of the Gait Cycle
| Phase of Gait Cycle | Description |
|---|---|
| Stance Phase | |
| Initial contact | The instant the foot contacts the ground |
| Loading response | From flat foot position until the opposite foot is off the ground for swing |
| Midstance | From the time the opposite foot is lifted until the ipsilateral tibia is vertical |
| Terminal stance | From heel rise until the opposite foot contacts the ground (contralateral initial contact) |
| Preswing | From initial contact of the opposite foot and ends with ipsilateral toe-off |
| Swing Phase | |
| Initial swing | Begins with lift-off of the foot from the floor and ends when the foot is aligned with the opposite foot |
| Midswing | Begins when the foot is aligned with the opposite foot and ends when the tibia is vertical |
| Terminal swing | Begins when the tibia is vertical and ends when the foot contacts the ground (initial contact) |
In the laboratory, gait can be studied through the collection of a wide range of information. Four primary components of quantitative gait analysis (Box 5-2) can be recorded:
Kinematics
Temporal and Spatial Descriptive Measures
Available techniques include the simple use of ink and paper, foot switches, and instrumented walkways to the most sophisticated systems that require the patient to be instrumented (which can provide considerable additional data). One example of a system that requires no patient instrumentation is the Electronic Gait Mat II. This instrumented walkway measures 3.8 m in length and contains approximately 10,000 electronic switches, scanned at 100 Hz. Patients can use gait aids or shoes and braces, if necessary, as they walk over the mat, which ideally is mounted flush with the floor. A recording of foot contact generates a timed “electronic footprint.” A printout that provides calculated data about walking speed, cadence, stance, and swing times for each foot, as well as stride lengths, step lengths, and the width of the base of support, is generated.6,25 The data can be easily stored for future reference or to perform other data analysis.9 Comparing left- and right-side data from one subject can be used to determine the extent of unilateral impairment. Comparisons can also be made with normative gender, age, and walking speed–matched data. This allows inference of the level of dysfunction.
Motion Analysis
Video and passive optoelectronic systems use retroreflective markers applied to the subject. The markers are “illuminated” by an external power source and are tracked by the detectors (camera). Near-automatic marker identification and digitization are reliable if marker paths do not cross, as can usually be expected for standard marker placements in normal walking. However, conversion into quantitative data might require some manual intervention for marker identification in pathologic gait, where increased limb rotation, sudden motions, or crossover of segment paths can occur. Manual digitization and tracking of the raw data can be in some instances time-consuming and error-prone.4,6,22 With active optoelectronic systems, each marker is self-illuminated (hence the designation “active”). No postcollection marker identification is needed because time sequencing between marker illumination and detector reception uniquely identifies each light-emitting diode.6 Each marker is activated at a slightly different (in the order of microseconds) instant in time. Telemetry (via infrared transmitters) in newer active systems such as the CODA CX1 (Charnwood Dynamics Ltd, Rothely, England) has eliminated the use of “umbilical cords” to power each marker. Not having to manually identify or track markers, and the real-time nature of these systems are advantages over the passive marker systems.
Kinetics
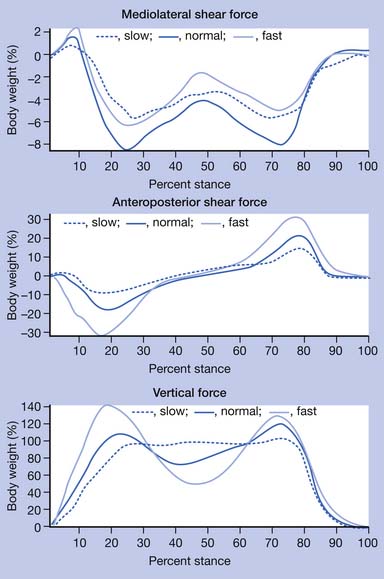
Kinetic analysis deals with the forces that are produced during walking. Sir Isaac Newton described basic but critical concepts that are useful in understanding the effect of gravity on gait. He stated in his third law of motion that “for every action there is an equal and opposite reaction.” This concept indicates that, as long as gravity is present, there is a reaction force where the body interacts with the ground. The ground reaction force is a reflection of the body weight and acceleration. This force can be resolved into a convenient set of directions, such as vertical, anteroposterior, and mediolateral (Figure 5-4). The anteroposterior shear forces are sometimes referred to as propulsion and breaking forces, respectively. Friction is responsible for the generation of shear forces. A force plate is a “sophisticated scale” that can measure vertical (downward force similar to the body weight registered on a scale) as well as shear forces, which are those acting in the plane of the floor secondary to friction. Triaxial force plates measure the total force (a vector summation of all three components) acting on the center of pressure (a focal point under the foot at which the force is idealized to be concentrated). Preferably two platforms placed adjacent to each other are used, so that the total force under each foot can be recorded independently and simultaneously. In most instances the force platforms are placed in the midpoint of the walkway and concealed in the floor so that steady-state, natural walking parameters are measured. Together the forces in all three directions measured by the force plates comprise the total force.
< div class='tao-gold-member'>
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


