The arthroscopic approach to hip pathology is rapidly becoming an accepted and common tool in the orthopedic surgeons’ armamentarium. Improvements in instrumentation, technique, and surgeons’ experience have made the minimally invasive treatment of multiple hip derangements possible. This chapter provides the novice hip arthroscopist with a detailed description of the indications, operative setup, and technique for performing hip arthroscopy.
BACKGROUND, PRESENTATION, AND INDICATIONS FOR HIP ARTHROSCOPY
Although rapidly gaining in popularity, hip arthroscopy is not a new procedure. For decades, few surgeons approached the hip arthroscopically as the procedure itself requires significant technical acumen and definitive diagnosis of hip pathology is sometimes difficult. The clinical symptoms and physical finding associated with hip pain may be varied and subtle. Diagnosis is often delayed by an average of 21 months as patients are referred to an average of 3.3 health care providers before reaching a hip arthroscopist. During that period, they have often undergone a variety of treatments including physical therapy, nonsteroidal anti-inflammatory or narcotic medications, or other surgery including spine, ovary, or hernia exploration.
Not all pain believed to be emanating from the hip is actually intra-articular hip pain. The numerous anatomic structures in the vicinity of the hip joint may confuse the clinical presentation. Presentation of intraarticular hip pain is most commonly groin pain with or without radiation to the knee, pain localized by the patient with his or her hand encircling the lateral hip above the greater trochanter with the thumb posterior and fingers in a C-shape (C-sign), mechanical clicking or pinching in the groin, or pain with sitting and getting in and out of the car. The presence of mechanical symptoms in addition to groin pain is a favorable prognostic factor with more than 85% improvement postoperatively (34) Intra-articular hip pain is not lateral pain over the greater trochanter, buttock/posterior leg pain or palpable hip girdle tenderness (Table 45.1).
Proper patient selection is paramount in achieving a successful outcome from arthroscopic hip surgery. In addition to the history and physical, a focused exam, as summarized in Table 45.2, provides valuable clues for localizing pathology.
Perhaps the most important tools in evaluating the hip are plain radiographs. Table 45.3 summarizes important radiographs and the measurements they provide.
In addition, the Dunn or elongated-neck lateral (performed with the hip in 90 degrees of flexion and 20 degrees of abduction) may be used to further identify femoral neck offset. The False profile radiograph, with the patient rotated 65 degrees and the beam perpendicular to the hip, demonstrates anterior osseous coverage of the hip.
When history, physical and plain radiographs indicate intra-articular pathology, the final two steps in preoperative diagnosis are MR Arthrogram (MRA) and diagnostic injection with analgesics (Figs. 45.1, 45.2 and 45.3). Soft tissues of the hip should be visualized using MRA in most clinical settings. Figures 45.4, 45.5 and 45.6 demonstrate common MRA views. While some institutions report the ability to visualize these structures adequately without the addition of contrast, in most settings, the addition of contract is vital. MRA has 90%/91% sensitivity and accurate for detecting hip pathology, while plain MRI has only 30%/36% sensitivity and accuracy (1). Finally, confirmation of intra-articular pathology as the source for hip pain is obtained via intra-articular injection. At the time of MRA, a mixture of lidocaine (6 mL 1%), marcaine (6 mL 0.25%), and kenalog (80 mg) is injected into the joint. The patient is then asked to perform the activities that normally cause pain to the hip and report the degree of relief from these symptoms within the first 3 hours following injection. The amount of relief from this diagnostic injection within the first 3 hours following injection is 90% predictive of the relief the patient can expect postoperatively.
TABLE 45.1 Summary of Hip Symptoms Associated with Labral Tears
Onset of symptoms
Insidious
61%
Acute
30%
Trauma
9%
Intensity
Moderate/severe
86%
Location
Groin
92%
Ant. thigh/lateral hip/buttock
Quality of pain
Sharp
86%
Dull
80%
Combination sharp/dull
70%
Activity related
91%
Night pain
71%
Mechanical symptoms
53%-77%
Pain during walking
70%
Pain during pivot
70%
Source: Adapted from J Bone Joint Surg. 2005;88-A:1450.
TABLE 45.2 Focused Physical Exam of the Hip
Exam Name
Exam Indication
Gait
Antalgic—pain/trendelenberg—gluteal weakness
Trendelenberg sign
Gluteal weakness
Palpation (groin, lateral hip, buttocks)
Intra-articular pathology generally not palpable
Strength (hip flexors/abd/add)
Thomas sign
Tight hip flexors
Range of motion
Flex—FAI, ER—tight hip capsule, IR—OA
Log roll/heel strike
Intra-articular pathology/fracture
Scour test
Labral tear
FADIR
Impingement ± popping/clicking
FABER (location important)
SI joint/iliopsoas/FAI
TABLE 45.3 Radiographic Evaluation of the Hip
Radiograph
Measurement
AP WB pelvis
CEA—dysplasia
<20 under coverage
20-40 normal
>40 pincer lesion
Tonnis angle
<10 degrees normal
>10 degrees increased lateral contact pressures
Cross over sign—anterior rim crosses in front of posterior rim indicating retroversion of the acetabulum
AP hip
Cross table lateral
CAM—decreased femoral neck offset
Hip arthroscopy is indicated when patients present with persistent pain that is unrelieved by thorough physical therapy and reproducible by physical exam, are nonresponsive to conservative measures, and have documentation of intra-articular pathology by MRA and positive relief from intra-articular injection within the first 3 hours after injection.
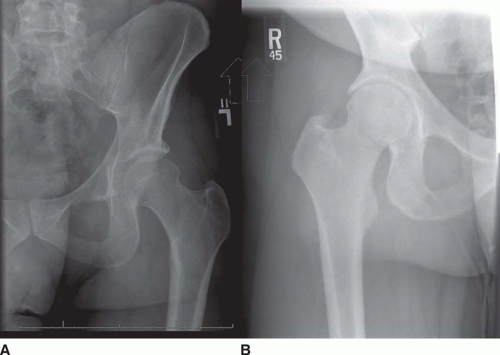
FIGURE 45.1 AP pelvis without crossover sign.
FIGURE 45.2 A: AP hip with normal CEA B: AP hip with Pincer lesion.
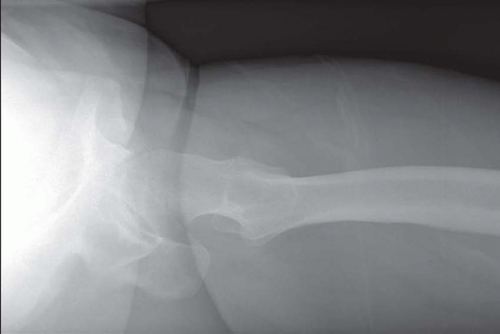
FIGURE 45.3 Cross table lateral with CAM lesion.
In recent years, much focus has illuminated the pathology behind labral tears. Though the pain associated with a torn labrum is often the inciting reason patients seek medical care, labral pathology itself is the consequence of the primary underlying hip derangement. These pathology include femoral acetabular impingement (FAI), major or athletic hip trauma, capsular laxity/hip hyper mobility, hip dysplasia with a shallow center edge angle (CEA) of <20 degrees and subsequent hypertrophic labrum, iliopsoas impingement and snapping over the anterior pelvic rim and DJD with degeneration of the labrum as well as the cartilage. Detailed coverage of several of these topics appears in subsequent chapters and will be described in brief here.
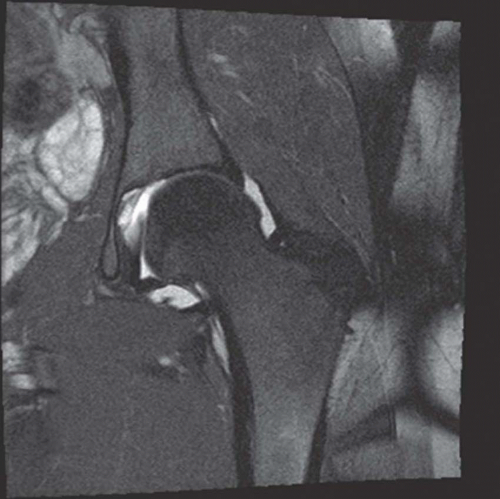
FIGURE 45.4 MRA axial oblique with labral tear.
FIGURE 45.5 MRA coronal.
Femoral acetabular impingement
First described in 1965 (25), FAI describes the repetitive abutment and subsequent microtrauma between the femoral neck and acetabular rim (Table 45.4). The impingement occurs as the femoral neck CAM lesion flexes against a normal or overhanging (high CEA) acetabulum and pushes the labrum up and away from the acetabular edge. This leads to labral tearing or fraying and is thought to eventually peel back the acetabular cartilage at the area of impact leading to early arthritis. The concept of optimal femoral neck offset is well known from the arthroplasy literature with too little offset leading to hip instability, with the head levering out of the cup, impingement, and wear. Historically, surgical management of FAI included periactabular osteotomy (30) and surgical dislocation (28). Now, FAI, including osteoplasty of the acetabular rim and femoral CAM lesion, is performed arthroscopically as described in following chapters.
Acetabular Dysplasia
Acetabular dysplasia is a part of a continuum of developmental disorders that includes FAI. While severe dysplasia cannot be treated by arthroscopy alone and requires open osteotomy, mild and moderate dysplasia may be. Acetabulum with CEA of 16 to 28 degrees is amenable to arthroscopic labral surgery (20). With the dysplasia, the labrum becomes hypertrophic in the anterior and superior regions and is more susceptible to tearing (14). In these cases, the labrum is repaired back down to acetabular rim. Developmental dysplasia is also associated hypertrophy of the ligamentum teres and increased wear with time causing impingement and pain. Débridement of the ligamentum and repair of the labrum in dysplasia demonstrate improved clinical outcomes (6
Only gold members can continue reading. Log In or Register to continue


 Arthroscopic Management of Elbow Osteochondritis Dissecans Lesions
Arthroscopic Management of Elbow Osteochondritis Dissecans Lesions



