Hip and Acetabulum
Bernard F. Morrey
Matthew C. Morrey
The basis of the development of this chapter deals principally with the surgical exposures that I and my partners have found useful to manage the majority of the pathology encountered at the hip. Exposures of the acetabulum and pelvis are treated in a separate chapter. Herein we discuss the more functional extensile exposures of the hip generally described as anterolateral, lateral (trochanteric), and posterolateral. Variations exist in each of these which are readily made and modified according to personal preferences once the principals of the exposures are known. In addition to these, three additional limited or minimally invasive exposures are presented. This chapter makes no effort to review every surgical exposure that has been described but those which are useful and relevant for managing the majority of hip problems.
I personally reject the term and even the concept of “minimally invasive” exposures and prefer the term “limited invasive” surgery. The reason is that this conveys to me the reasonable position to limit exposure as able and avoid unnecessary tissue damage but not minimize it at all cost. The three exposures detailed here all have value in that they are effective, have a low complication rate, and are relatively easy to perform. The criteria for the use of any of these exposures are:
Abbreviated learning curve
No increased complication rate
Minimal muscle injury
Facilitated rehabilitation
ANTERIOR-LATERAL EXPOSURE (HARDINGE) (1,2)
Indications
Hip joint replacement. Value of anterior exposures: typically more stable than posterior exposures.
Disadvantages
Strength of abduction is regained slower after an anterior compared to a posterior exposure (3).
Note: The Hardinge exposure is an example of the family of anterior lateral approaches and has some similarity to several other anterior lateral exposures including the Mayo limited approach discussed below. In general the anterior lateral exposures vary principally in the manner and effect of releasing the insertion of the gluteus medius while taking care to avoid the superior gluteal nerve which typically runs 3 to 5 cm proximal to the tip of the greater trochanter (Fig. 7-1).
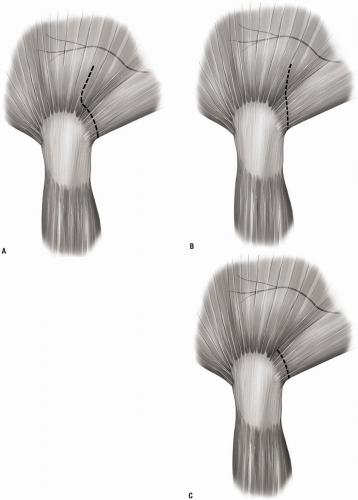 FIGURE 7-1 |
 FIGURE 7-2 |
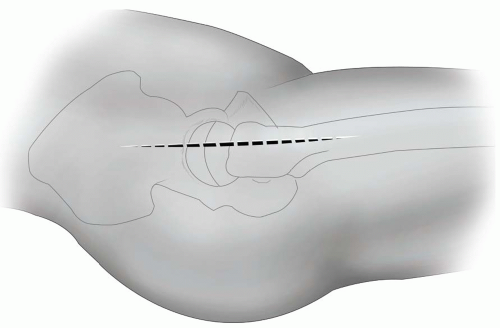 FIGURE 7-3 |
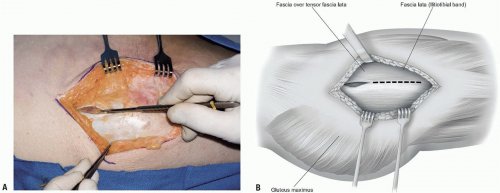 FIGURE 7-4 |
Position
The patient is placed and supported in the lateral decubitus position; however, the supine position is also acceptable (Fig. 7-2).
Technique
Skin incision: the 14 to 16 cm skin incision is centered over the greater trochanter and extends approximately 6 to 8 cm distally along the anterior aspect of the trochanter and down the anterior lateral aspect of the femoral shaft. Proximally, the skin incision extends 6 to 8 cm in line with the fibers of the gluteus maximus muscle (Fig. 7-3).
The iliotibial band is entered and split distally and the gluteus maximus muscle is split proximally. The gluteus maximus is retracted posteriorly and the tensor fascia lata retracted anteriorly (Fig. 7-4).
Note: If the gluteus is separated from the tensor fascia lata muscle at the site of their interface, the iliotibial band may need to be further released posteriorly to dislocate the hip.
The deep exposure begins at the anterior margin of the trochanter and extends distally to include the anterior third of the vastus lateralis muscle (Fig. 7-5). Proximally, the incision extends about 4 to 5 cm past the trochanteric tip and splits the gluteus medius musculature in line with its fibers separating its anterior one third from the posterior two thirds.
Note: Effort is made to maintain continuity of the anterior sleeve of muscle comprising the gluteus medius and anterior portion of the vastus lateralis.
The interval is developed by subperiosteally releasing the antero-oblique fibers of the gluteus medius from the trochanter in line with the remaining anterior fibers of the more proximally fanshaped portion of the medius musculature.
The anterior third of the vastus lateralis muscle is elevated from the trochanter and proximal femur for a distance of about 5 to 7 cm. The sleeve of tissue containing this portion of the abductors and the vastus lateralis is then reflected anteriorly and retracted with a narrow Hohlman retractor (Fig. 7-7A). This allows ready access to the anterior capsule (Fig. 7-7B).
The gluteus minimus muscle is detached from the trochanter beginning anteriorly and separated from the capsule to the extent needed for adequate exposure. A curved Hohlman retractor placed over the femoral neck facilitates retraction of the medius and minimus musculature.
The capsule is excised anteriorly, placed over the femoral neck, and further release of the lateral and inferior aspect of the capsule is performed as needed (Fig. 7-8).
The hip is dislocated by external rotation and flexion. For this exposure the leg may be placed in a sterile pocket anteriorly to prepare the femoral canal (Fig. 7-9).
Closure: After the procedure the musculature is closed with side-to-side running nonabsorbable sutures.
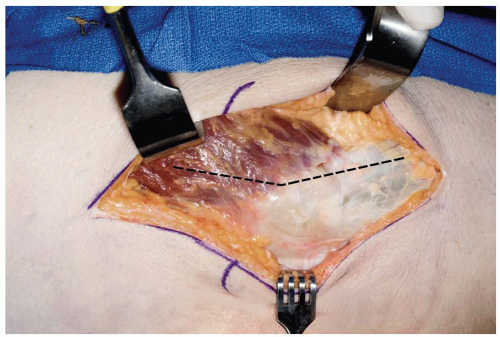 FIGURE 7-5 |
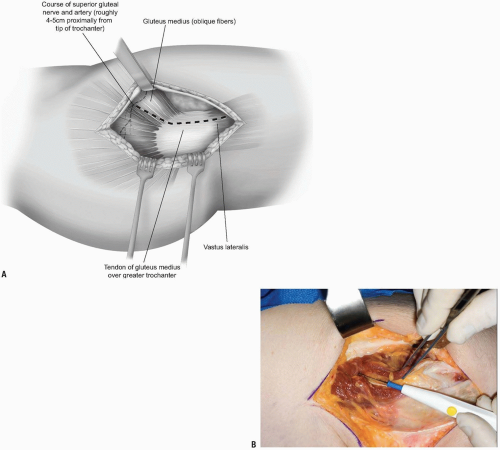 FIGURE 7-6 |
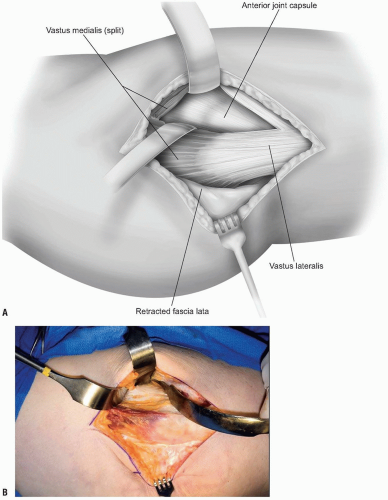 FIGURE 7-7 |
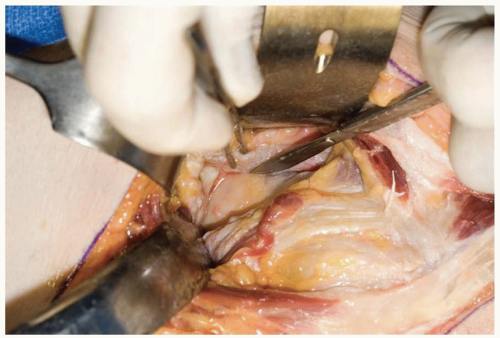 FIGURE 7-8 |
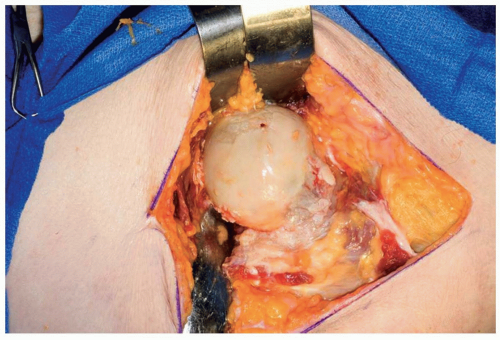 FIGURE 7-9 |
THE MAYO LIMITED (MINIMAL) ANTERIOR
This exposure was developed by the author in 1995. The goal was to preserve as much of the gluteus medius attachment as possible (Fig. 7-10). It is still preferred over the “minimally invasive” approaches currently being popularized as it satisfied the criteria noted at the beginning of the chapter.
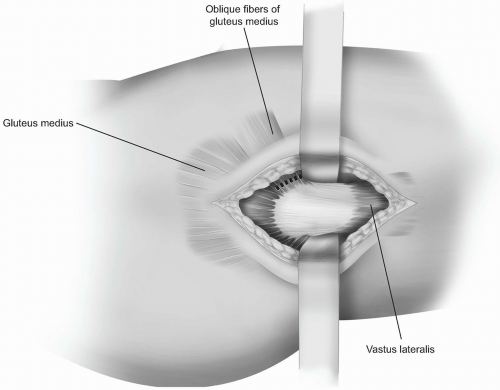 FIGURE 7-10 |
Indications
Anterior exposure to the hip joint: Incision and drainage; hip joint replacement, typically more stable than posterior exposures.
Position
The patient is placed in the lateral decubitus position. The pelvis is stabilized with method of choice, but should be well fixed vertical to the floor for hip joint replacement (Fig. 7-11).
Technique
Skin incision: an 8 to 10 cm skin incision is made just anterior to the midline of the trochanter with the distal one-third distal to the tip of the trochanter and the proximal two-thirds over the gluteus medius (Fig. 7-12).
Through this skin incision the tensor fascia lata is identified (Fig. 7-13) and split in the midline from the trochanter distally for a distance of approximately 7 cm. Proximally the muscle of the gluteus maximus is split or alternatively the interval between the gluteus maximus and the tensor fascia lata is identified and split for a distance of approximately an additional 6 cm (Fig. 7-14).
The fascia of the gluteus maximus is reflected posteriorly and the tensor fascia lata is retracted anteriorly.
The anterior inferior muscle fibers of the gluteus medius insert almost perpendicular to the long axis of the trochanter (Fig. 7-15). These “anterior-oblique” fibers of the gluteus medius are isolated (Fig. 7-16) and released with a cutting cautery leaving a cuff of attachment remaining on the trochanter.
The release proceeds proximally to the level of the tendinous portion of the gluteus medius and to the leading edge of the gluteus minimis (arrow) (Fig. 7-17).
Note: In tight hips a centimeter of the tendinous attachment of the gluteus at the anterior-superior corner of the trochanter may need to be released.
The released anterior-oblique fibers of the gluteus medius are reflected proximally and medially. The capsule is identified and is cleaned of soft tissue.
Note: The key to this exposure resides in the poorly documented or appreciated anatomic feature of the ability to expose the anterior capsule by releasing just those few anterior-oblique fibers.
A curved self-retaining retractor is placed between the gluteus minimus and the capsule. A wide self-retaining retractor is placed anteriorly over the rim of the acetabulum allowing ready access to the anterior capsule (Fig. 7-18).
The hip joint is entered in line with the femoral neck. The anterior portion of the capsule is excised. The inferior capsule is released. The knife is passed blindly over the lateral neck of the femur releasing the lateral capsule. The labrum is incised in several areas radial to its circumference (Fig. 7-19).
A bone hook is placed around the femoral neck. The hip is externally rotated and the femoral head is delivered into the wound (Fig. 7-20). For hip replacement the leg is placed on the table and externally rotated to expose the acetabulum.
Note: If difficulty of dislocation is encountered, the iliotibial band is released and allowed to slip posterior to the greater trochanter at the time of hip dislocation.
Closure: The author prefers to place sutures through the prepared femoral canal and at the margin of the greater trochanter for a transosseous purchase of the nonabsorbable no. 5 suture (Fig. 7-21). After reduction of the hip, these sutures are used to repair the antero-oblique fibers of the gluteus medius.
Note: Of significance is that the majority of the abductors has been left intact with this exposure and generally is not too damaged by femoral canal reaming.
Skin closure is routine (Fig. 7-22).
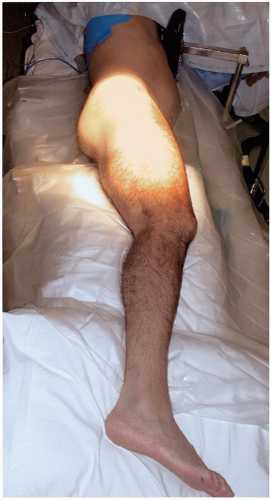 FIGURE 7-11 |
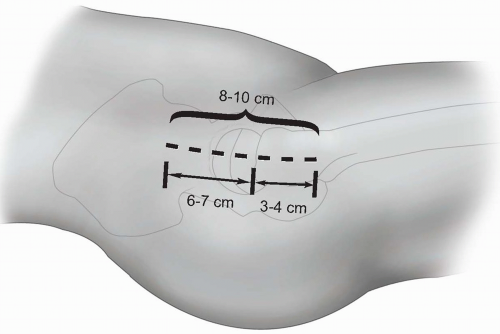 FIGURE 7-12 |
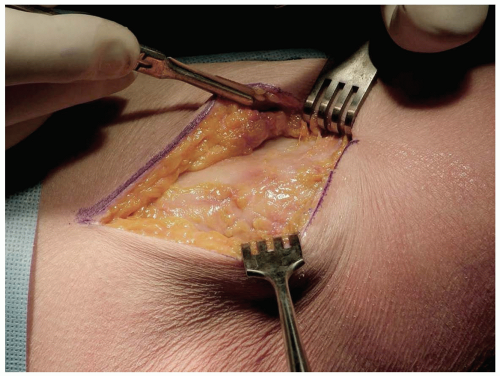 FIGURE 7-13 |
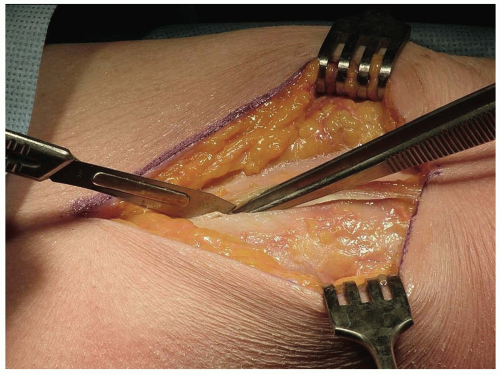 FIGURE 7-14 |
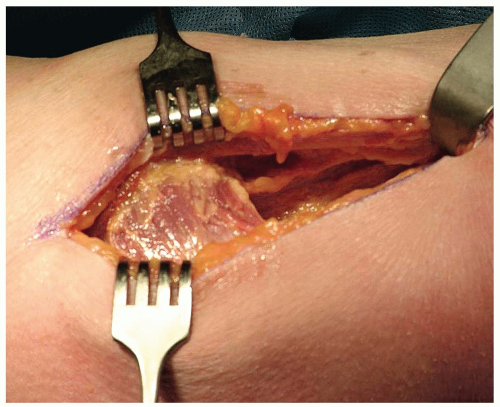 FIGURE 7-15 |
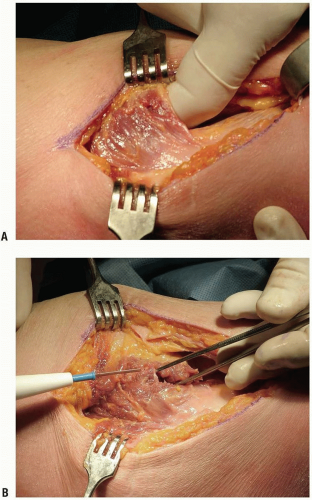 FIGURE 7-16 |
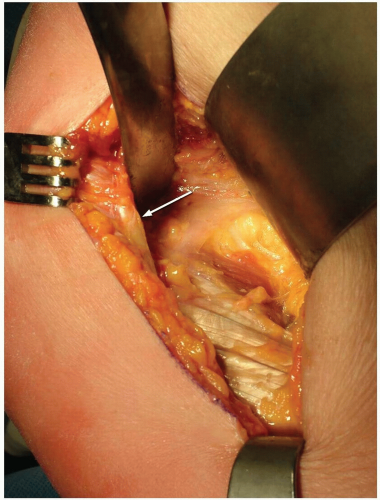 FIGURE 7-17 |
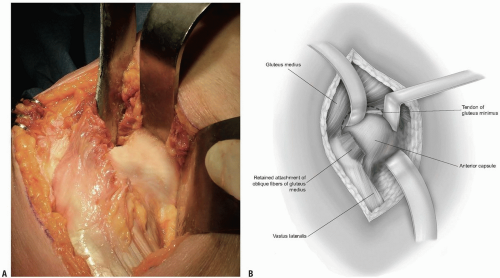 FIGURE 7-18 |
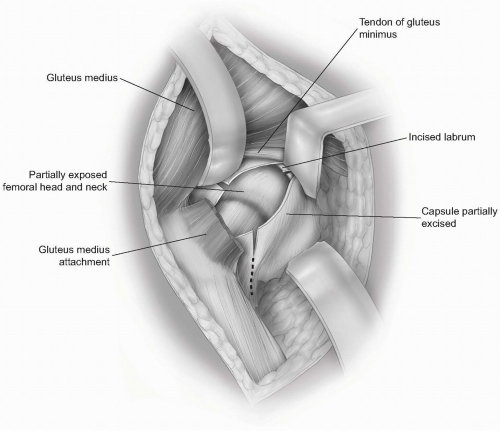 FIGURE 7-19 |
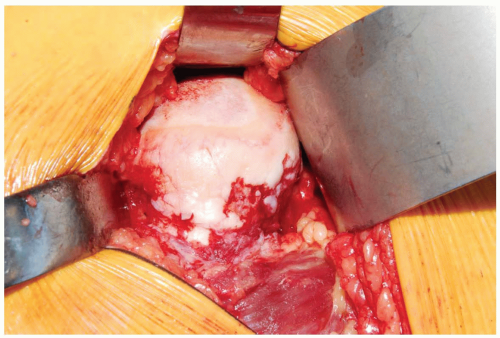 FIGURE 7-20 |
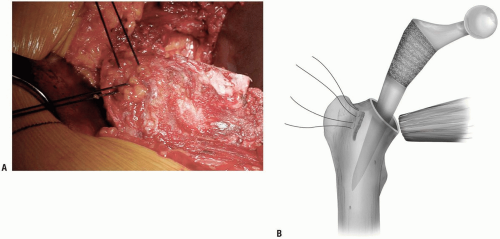 FIGURE 7-21 |
 FIGURE 7-22 |
LIMITED ANTERIOR HIP JOINT EXPOSURE (LIMITED SMITH-PETERSON) (5)
Indications
One of the minimally invasive muscle sparing techniques for hip joint replacement, or for any anterior joint arthrotomy.
Position
The patient is placed supine on the operating table.
Technique
The skin incision begins two finger-breadths below the anterior-superior iliac spine (Fig. 7-23A) and extends distally for approximately 8 cm in a linear fashion between the tensor fascia lata and the sartorius (Fig. 7-23B)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








