Hand and Wrist
PART 1. Dorsal Approach to the Wrist Joint
Julie E. Adams
Scott P. Steinmann
Dorsal approaches to the wrist joint are useful to address fractures, dislocations, ligamentous injuries, arthritis, and other pathology such as congenital anomalies or neoplasms (1, 2, 3). Moreover, one can perform compartment releases, tenosynovectomy, and posterior interosseous nerve (PIN) neurectomy through a dorsal approach (1,4).
ANATOMIC CONSIDERATIONS
The superficial nature of the wrist relative to the dorsum of the hand facilitates easy exposure (2). The dorsal aspect of the wrist is characterized by a loose skin and subcutaneous tissue. A thin superficial fascia covers the dorsal aspect of the wrist and hand including fatty and fibrous layers, cutaneous nerves, and venous and lymphatic vessels. When approaching the wrist joint, the vessels should be preserved whenever possible to facilitate venous return from the hand which is largely dependent upon these cutaneous vessels (3). The dorsal nerves and subcutaneous veins should be raised in continuity with the skin and subcutaneous tissues. The dorsal aspect of the hand is supplied by branches of the superficial branch of the radial nerve and the dorsal sensory branch of the ulnar nerve in a variable pattern with an inconsistent contribution of the lateral and posterior antebrachial cutaneous nerves (5, 6, 7). These cutaneous nerves should be identified and preserved. Use of vessel loops to isolate and protect the nerves may be helpful.
The extensor retinaculum is the next deepest structure encountered. The wrist and finger extensors travel beneath the extensor retinaculum in six dorsal compartments, delineated by fibrous septae attaching from the extensor retinaculum to the periosteum of the radius. Palmer et al investigated the anatomy and biomechanical role of the extensor retinaculum of the wrist (8). This fibrous thickening of the antebrachial fascia lies in a band over the dorsal aspect of the wrist joint and is continuous with the volar carpal ligament palmarly and the dorsal fascia over the distal hand and metacarpal region (8). Fibrous septae traversing from the retinaculum palmarly to insert upon the radial periosteum or wrist capsule create five fibro-osseous tunnels and one fibrous canal, the 5th compartment. From radial to ulnar, the compartments are as follows: first dorsal compartment: abductor pollicis longus and extensor pollicis brevis; second dorsal compartment: extensor carpi radialis longus and brevis; third dorsal compartment: extensor pollicis longus; fourth dorsal compartment: extensor digitorum communis and extensor indicis proprius; fifth dorsal compartment: extensor digiti minimi; and sixth dorsal compartment: extensor carpi ulnaris.
Deep to the extensor tendons lies the capsule of the wrist joint. The capsule is comprised of ligamentous tissue and nonligamentous tissues. The major dorsal wrist ligaments are the dorsal radioulnar ligament, the dorsal radiocarpal ligament, and the dorsal intercarpal ligament. The dorsal radioulnar ligament spans from the radius at the dorsal margin of the sigmoid notch over the distal radioulnar joint (DRUJ) to attach to the head of the ulna and along the styloid process. It contributes to the extensor carpi ulnaris subsheath and the triangular fibrocartilaginous complex (TFCC). Similarly, the dorsoradioulnar ligament attaches to the radius at a site ulnar to the Lister’s tubercle then spans the radiocarpal joint obliquely to attach to the dorsal horn of the lunate and to form the lunotriquetral interosseous ligament superficially. The dorsal intercarpal ligament is confluent with the dorsal radiocarpal ligament at their insertions upon the triquetrum. It courses distally and obliquely from the triquetrum to the dorsal ridge of the distal half of the scaphoid and to the dorsal cortex of the trapezoid (2). To expose the dorsal aspect of the wrist, a dorsal capsular flap (the Mayo flap) can be raised by elevating a split dorsal radiotriquetral and dorsal intercarpal ligament with a radial based flap.
DORSAL SURGICAL APPROACH
Position
The patient is positioned in the supine position with the forearm pronated. The arm is exsanguinated and a tourniquet inflated.
Landmarks
Superficial landmarks are palpable. The radial styloid lies in a lateral position when the hand and forearm are in the anatomic position. The ulnar styloid process is medially and posteriorly located when the hand and forearm are in the anatomic position. The extensor carpi ulnaris (ECU) lies in a dorsal groove radial to this landmark. Distally, the eight carpal bones are aligned in two rows. The anatomic snuff box is outlined when the thumb is abducted. The scaphoid bone lies in the floor and ulnar deviation of the wrist causes it to slide outward from beneath the radial styloid to become palpable. Lister’s tubercle or the dorsal tubercle of the radius lies about one third the distance across the dorsum of the wrist from the radial styloid. The scaphoid-lunate junction (and scapholunate ligament) is located just distal to Lister’s tubercle. The capitate lies at the base of the 3rd metacarpal bone. When the wrist is in a neutral position, the depression in the capitate becomes palpable (9).
Technique
The skin incision may be longitudinal or transverse. We prefer a longitudinal incision that may be extended distally and proximally (3,10) (Fig. 1-1). The incision may be centered in the radial and ulnar dimension and extends longitudinally from 2 to 3 cm proximal to the radiocarpal joint to 2 cm distal to Lister’s tubercle, depending on the pathology to be addressed. Although not in Langer’s lines and indeed, the longitudinal incision is perpendicular to Langer’s lines, incisional contracture is not problematic as the skin overlying the dorsum of the wrist is quite pliable and longitudinal scarring is uncommon. Alternatively, a transverse slightly curved incision, directed in line with Langer’s lines, with the concavity oriented distally may be used (2) (Fig. 1-2). This incision can extend from the radial styloid to the ulnar styloid, in which case mobilization of the incision allows for exposure of the carpometacarpal joints and the distal radial metaphysis (2).
Full-thickness flaps are developed down to the extensor retinaculum (Fig. 1-3), taking care to identify and preserve the superficial radial nerve, the dorsal sensory branch of the ulnar nerve, and any dorsal veins, and elevating them with the flaps (2,3). This is in contradistinction to the practice on the palmar aspect of the hand, where skin flaps are raised and elevated away from the neurovascular structures.
If the pathology to be addressed is in the extensor tendons, the retinaculum over the desired compartment is incised. If a posterior interosseous nerve (PIN) neurectomy is to be performed, a deeper dissection is made 2 cm proximal to the extensor retinaculum (11) (Fig. 1-4). The dissection proceeds through the deep fascia of the forearm. The PIN is identified as it enters the 4th extensor compartment and a 2 cm segment of the nerve, which is purely sensory at this level, is excised (11) (Figs. 1-4 and 1-5). The PIN and posterior interosseous artery course longitudinally from proximal to distal. Proximally, the PIN innervates the extensor pollicis longus (EPL) and extensor indicis proprius (EIP). At this level, it departs from the posterior interosseous artery and travels distally bound under a fascial layer to the interosseus membrane along the ulnar border of the radius (4). At the level of the Lister’s tubercle, the PIN lies adjacent to the ulnar origin of the 3rd dorsal compartment. It then travels distally with the anterior interosseus artery across the radiocarpal joint. At the level of the scapholunate ligament, the PIN branches into its terminal extensions to bring sensory and proprioceptive nerve fibers to the capsule and ligaments of the dorsal aspect of the wrist (4). By denervating the PIN (and anterior interosseus nerve [AIN]), pain related to the scapholunate ligament and adjacent capsule may be attenuated.
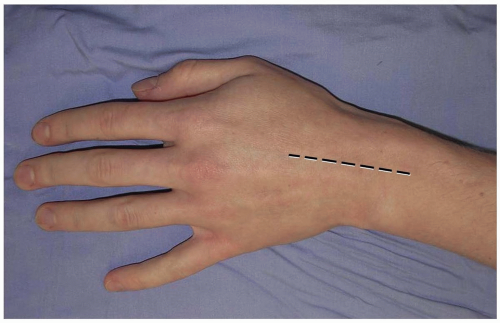 FIGURE 1-1 A longitudinal incision centered over the wrist is preferred. Incisional contractures are rarely problematic. |
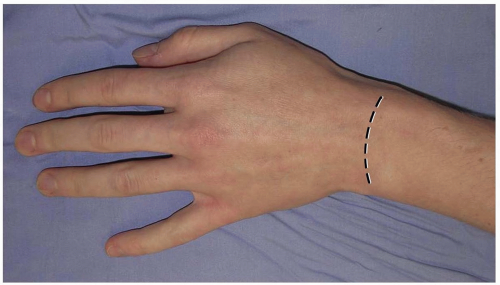 FIGURE 1-2 An alternative transverse incision in Langer’s lines. This incision can extend from the radial styloid to the ulnar styloid, in which case mobilization allows for exposure of the carpometacarpal joints and the distal radial metaphysis. |
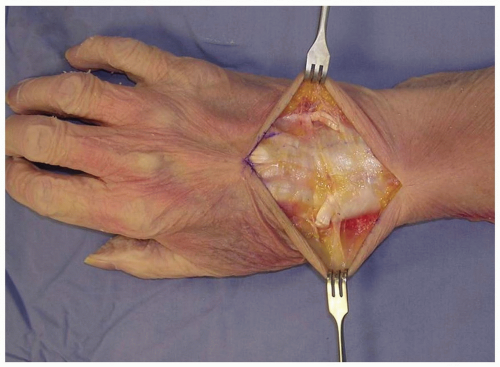 FIGURE 1-3 Full-thickness flaps are developed down to the extensor retinaculum, taking care to identify and preserve the superficial radial nerve, the dorsal sensory branch of the ulnar nerve, and any dorsal veins, and elevating them with the flaps. EDC (extensor digitorum comminus), EDM (extensor digiti minimi), EPL (extensor pollicis longus). |
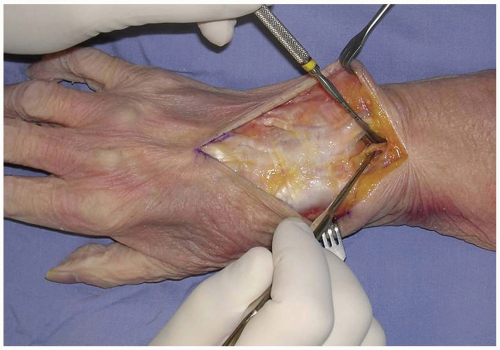 FIGURE 1-4 The posterior interosseous nerve (PIN) may be exposed for neurectomy by dissection 2 cm proximal to the extensor retinaculum. |
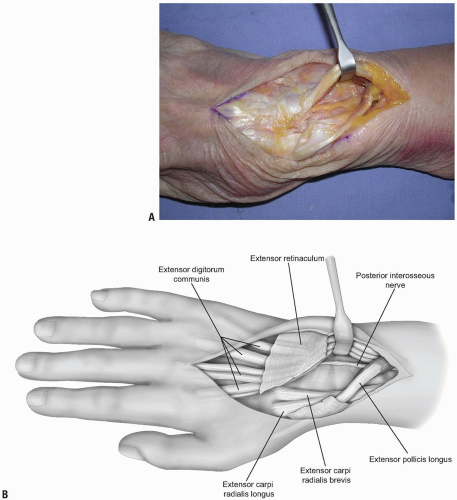 FIGURE 1-5 A,B: The PIN is identified as it enters the 4th extensor compartment and a 2 cm segment of the nerve, which is purely sensory at this level, is excised to achieve PIN neurectomy. |
To gain access to the wrist joint, the retinaculum overlying the 3rd dorsal compartment is incised longitudinally from the deep antebrachial fascia proximally and then distally to the distal margin of the retinaculum (Fig. 1-6). The EPL in the 3rd dorsal compartment is retracted radially, and the 4th extensor compartment is elevated subperiosteally or by dividing the septum between the 3rd and 4th compartments and reflecting the retinaculum as an ulnarly based flap (Fig. 1-7). The approach is limited by the septum between the 5th and 6th dorsal compartments. Radially, the extensor retinaculum may be elevated off of Lister’s tubercle and the 2nd dorsal compartment released. Subsequently, the extensor carpi radialis brevis (ECRB) and extensor carpi radialis longus (ECRL) can be retracted radially deep to the extensor retinaculum, with the EPL retracted radially and superficial to the extensor retinaculum. This allows for exposure of approximately 90% of the dorsal wrist (2) (Fig. 1-8).
The wrist capsule is divided and reflected to gain access to the pathology to be addressed. Care should be taken when planning the capsulotomy to access the wrist joint. A poorly designed capsulotomy may destabilize the joint by disrupting the dorsal capsular ligaments, result in limited range of motion due to scar formation, or leave inadequate remaining tissue to facilitate closure (2). While some surgeons advocate a simple transverse or longitudinal capsulotomy in line with the skin incision (and these may be adequate in revision surgery, subtotal or complete wrist fusion, or in other cases) (1,3,10), we prefer a ligament-sparing capsulotomy with capsulotomy incisions parallel to the dorsal wrist ligaments.
Radial Capsulotomy
The radial capsulotomy provides exposure of the radial two-thirds of the radiocarpal joint and most of the midcarpal joint. The fibers of the dorsal radiocarpal and dorsal intercarpal ligaments are incised in line with their fibers in the midline of each ligament (Fig. 1-9) with continuation along the dorsal rim of the radius toward the radial styloid process to generate a three-sided trapezoidal flap remaining attached on the radial side. The flap of capsule is then elevated sharply off the dorsal surface of the triquetrum then off the lunate and scaphoid, with care taken to avoid injury to the lunotriquetral and scapholunate interosseous ligaments (Fig. 1-10). Elevation is halted upon encountering the dorsal ridge of the scaphoid to avoid damage to the vascular supply of the scaphoid.
 FIGURE 1-6 To gain access to the wrist joint, the retinaculum overlying the 3rd dorsal compartment is incised longitudinally from the deep antebrachial fascia proximally and then distally to the distal margin of the retinaculum. |
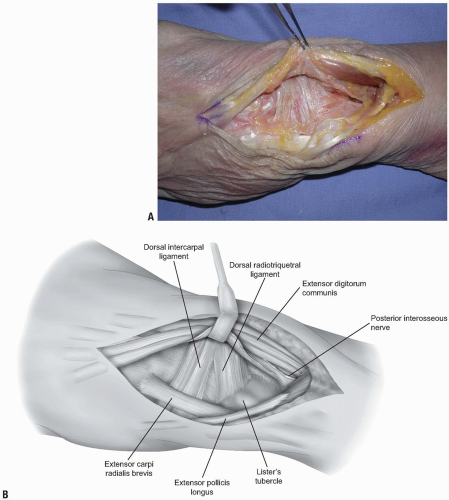 FIGURE 1-7 A,B: The EPL in the 3rd dorsal compartment is retracted radially, and the 4th extensor compartment is elevated subperiosteally or by dividing the septum between the 3rd and 4th compartments and reflecting the retinaculum as an ulnarly based flap. |
 FIGURE 1-8 The ECRL can be retracted radially deep to the extensor retinaculum, with the EPL retracted radially and superficial to the extensor retinaculum. This allows for exposure of approximately 90% of the dorsal wrist. |
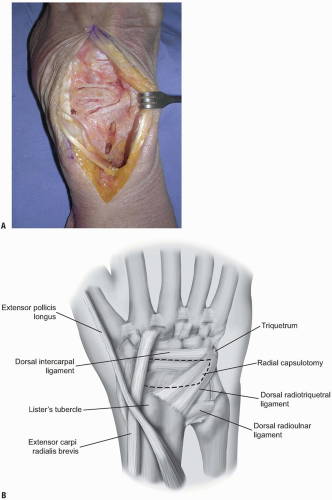 FIGURE 1-9 A,B: The fibers of the dorsal radiocarpal and dorsal intercarpal ligaments are incised in line with their fibers in the midline of each ligament, with continuation along the dorsal rim of the radius toward the radial styloid process to generate a three-sided trapezoidal flap remaining attached on the radial side. The flap of capsule is then elevated sharply off the dorsal surface of the triquetrum then off the lunate and scaphoid, with care taken to avoid injury to the lunotriquetral and scapholunate interosseous ligaments. |
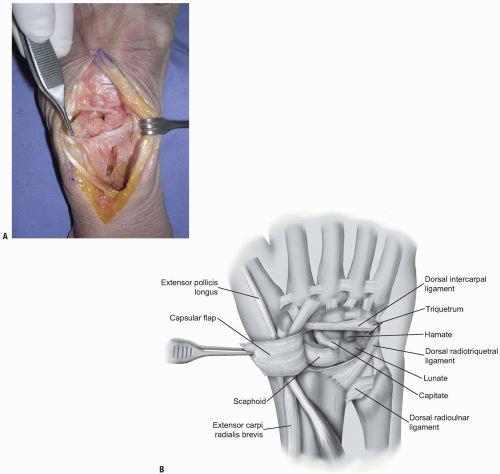 FIGURE 1-10 A,B: Elevation of capsular flaps in this manner preserves the blood supply and allows for closure of tissues following the procedure. |
Any loose synovial tissue is removed to allow for visualization of the lunate, the scaphoid, the scapholunate ligament, the dorsal aspect of the radiocarpal joint, the lunotriquetral joint, the proximal capitate and triquetrum, and the hamate. Mobilization radially allows for access to the proximal trapezoid, trapezium and STT joint. Distraction of the wrist allows for access to the palmar joint capsule of the radiocarpal joint and the midcarpal ligaments (2). Closure of the capsule is facilitated using 3-0 braided absorbable sutures in a figure of eight or horizontal mattress pattern (2).
Ulnar Capsulotomy
This approach allows access to the proximal lunate and triquetrum and the ulnar aspect of the radiocarpal joint. The skin and subcutaneous dissection may proceed as outlined above for the capsulotomy to the radial aspect of the joint (2). Alternatively, only the ulnar half of the transverse incision
may be made with dissection proceeding to the extensor retinaculum where the 5th extensor compartment is incised and the EDM retracted ulnarly. To expand the exposure, the septum between the 4th and 5th dorsal compartments may be incised, the 4th compartment entered and the extensor digitorum communis (EDC) and EIP tendons retracted radially.
may be made with dissection proceeding to the extensor retinaculum where the 5th extensor compartment is incised and the EDM retracted ulnarly. To expand the exposure, the septum between the 4th and 5th dorsal compartments may be incised, the 4th compartment entered and the extensor digitorum communis (EDC) and EIP tendons retracted radially.
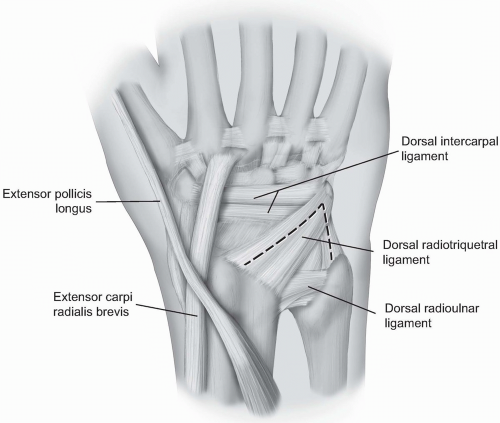 FIGURE 1-11 For the ulnar capsultomy, the dorsal radiocarpal ligament is incised longitudinally through its midline. The dorsal radioulnar ligament is preserved as are the 6th extensor compartment and the ECU subsheath. |
For exposure, the septum between the 5th and 6th compartments is identified at the level of the triquetrum and reflected ulnarly or the ulnar part of the extensor retinaculum is released radial to ulnar from Lister’s tubercle to the 6th extensor compartment.
The dorsal radiocarpal ligament is incised longitudinally through its midline (Fig. 1-11). The dorsal radioulnar ligament is preserved as are the 6th extensor compartment and the ECU subsheath. A proximally based triangular flap is elevated sharply from the triquetrum and the lunate, until the distal extent of the dorsal radioulnar ligament is encountered (Fig. 1-12). Synovial tissue is removed to expose the lunate, the lunotriquetral interosseous ligament, the triquetrum, and the triangular fibrocartilage complex (Fig. 1-13). Wrist distraction provides access to the ulnolunate and ulnotriquetral ligaments. Following completion of work, capsular closure is performed in the usual fashion with interrupted figure of eight or horizontal mattress sutures with 3-0 braided absorbable sutures (2).
SUMMARY
Dorsal exposure of the wrist joint is useful for procedures to address pathology of the carpus, the extensor tendons, the PIN, or fractures. The subcutaneous location makes this approach readily available and relatively simple. Attention to ligament sparing capsulotomy can preserve stability and motion in certain cases.
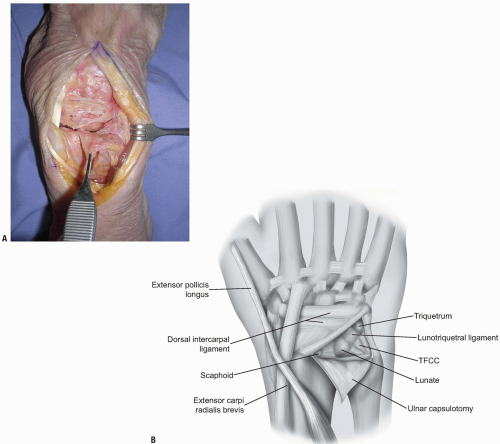 FIGURE 1-12 A,B: A proximally based triangular flap is elevated sharply from the triquetrum and the lunate, until the distal extent of the dorsal radioulnar ligament is encountered. |
 FIGURE 1-13 Synovial tissue is removed to expose the lunate, the lunotriquetral interosseous ligament, the triquetrum, and the triangular fibrocartilage complex. |
PART 2. Surgical Approach of the Ulnar Nerve at the Level of the Wrist
David Ruch
Nikolaos P. Zagoreos
The ulnar nerve runs down the volar surface of the forearm under the muscle and the tendon of the flexor carpi ulnaris (FCU) with the ulnar artery being on its radial side. Just before the wrist crease, the ulnar artery and nerve emerge from under the muscle and enter the distal ulnar tunnel canal in the wrist. At this level, the ulnar artery and nerve are located on the radial surface of the FCU.
The distal ulnar tunnel was initially described by Guyon, a French urologist, in 1861 and is also referred as Guyon’s canal (1). It is essentially a triangular fibro-osseous tunnel about 3 cm long located at the carpus. The volar carpal ligament forms the roof of the canal, which is a condensation of the forearm fascia and expansion of the FCU. The transverse carpal ligament, extending between the pisiform and the hook of the hamate, forms the floor of the canal. The hook of the hamate and the medial side defines the lateral side of the canal by the pisiform. The contents of the distal ulnar tunnel are the ulnar nerve, the ulnar artery, and the ulnar veins.
The roof of the canal is a very thin layer of tissue located quite superficially, exactly below the skin and the subcutaneous tissue. The respective roof of the neighboring carpal tunnel, the transverse carpal ligament, is the floor of the Guyon’s canal and is a relatively thick fibrous layer.
The longitudinal axis of the distal ulnar tunnel is angulated medially about 30 degrees to the long axis of the forearm and the wrist, since the hook of the hamate lies a little more distal to the pisiform.
Indications for volar approach of the ulnar nerve in the wrist are traumatic injuries of the ulnar nerve, compression neuropathies within the Guyon’s canal, and intrinsic muscle spasticity requiring ulnar motor neurectomy.
EXPLORATION OF THE ULNAR NERVE WITHIN THE GUYON’S CANAL
Regional or general anesthesia is routinely used and the exploration is performed in a bloodless field provided by a tourniquet. The ulnar nerve can be explored through a volar approach, which is located 1 to 2 cm more medially than the typical approaches for open release of the carpal tunnel. A consideration in planning the skin incision is the location of the palmar cutaneous branch of the ulnar nerve. Although this nerve was found to be present in only 25% in previous cadaveric studies (2), injury to it can lead to painful neuromas. The ideal incision should be located in the internervous plane between the palmar cutaneous branch of the ulnar and median nerve. Unfortunately, cadaveric studies have identified that there is not such a plane. This plane is innervated by the nerve of Henle (the nerve of the ulnar artery) and multiple ulnar cutaneous branches (3). Therefore, the dissection of the skin and subcutaneous tissue should be performed carefully, possibly under loop magnification, preserving any emerging cutaneous branches.
Anatomic landmarks are the pisiform, the hook of the hamate, and the hypothenar eminence. The typical incision is curvilinear in shape with the distal limb following the radial limb of the hypothenar eminence and the proximal limb extending on the volar ulnar part of the forearm. The wrist crease should not be crossed longitudinally but rather in an angle of 60 degrees to avoid skin contractures. The total length of the incision is about 6 to 8 cm centered over the wrist crease (Fig. 1-14).
The ulnar nerve and artery can be easily identified in the proximal part of the incision where they lie on the lateral surface of the tendon of the FCU (Fig. 1-15). They can be traced easily distally incising all tissues more superficial to these structures. The dissection of the subcutaneous fat should be performed bluntly in order to avoid injury to any cutaneous branches. The palmaris brevis muscle is elevated slightly ulnarly and the volar carpal ligament and pisohamate ligament are incised resulting in a complete decompression of the Guyon’s canal. The two branches of the ulnar nerve at the level of the pisiform are identified.
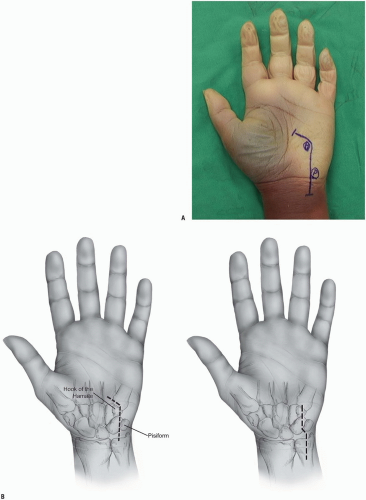 FIGURE 1-14 A,B: Incisions for the exploration of the ulnar nerve. At the level of the wrist, the incisions pass radial to the pisiform and ulnar to the hook of the hamate. |
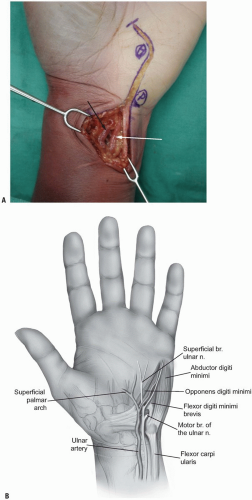 FIGURE 1-15 A,B: The ulnar artery (white arrow) and the ulnar nerve (black arrow) are identified at the radial margin of the flexor carpi ulnaris tendon. |
The motor branch is more dorsal and more medial at the level of the bifurcation. It can be traced beneath the fibrous arch of the hypothenar muscles formed between the abductor digiti minimi and the flexor digiti minimi, through the muscle mass of the opponens digiti minimi and around the hook of the hamate. A careful exploration of the floor of the distal ulnar tunnel is performed looking for any pathology like ganglions, fibrous bands, anomalous muscle masses, fractures of the hook of the hamate, and vascular aneurysms.
The tourniquet should be deflated before closure of the wound and the ulnar artery and its branches should be examined for any injury. Thorough hemostasis should be achieved since a post-operative hematoma can result in compression neuropathy of the ulnar nerve.
An alternative surgical approach is through an open carpal tunnel syndrome incision extending slightly more proximally and distally. The ulnar nerve and artery are located on the volar medial surface of the transverse carpal ligament and can be identified tracing the superficial palmar arch proximally. Several hand surgeons prefer to decompress the Guyon’s canal and the carpal tunnel simultaneously.
ANATOMY OF THE ULNAR NERVE IN GUYON’S CANAL
Around the pisiform the ulnar nerve divides into two branches, the superficial and the deep branch. The superficial branch gives immediately after the bifurcation motor branches to the palmaris brevis muscle and becomes purely sensory. It continues its course distally deep and medial to the ulnar artery providing sensory supply to the small finger and the ulnar side of the ring finger. The deep branch of the ulnar nerve bifurcation is purely motor and supplies the hypothenar muscles, all the interossei, the medial two lumbricals, and the adductor pollicis. The motor part of the ulnar nerve is located dorsally in the ulnar nerve at the level of the distal forearm and emerges from the nerve on the dorsal medial surface. The motor branch leaves the tunnel and passes beneath the fibrous arch of the hypothenar muscles and enters the interval between the abductor digiti minimi and flexor digiti muscles. It pierces the opponens digiti minimi and curves radially and dorsally around the distal part of the hook of the hamate, lying on the floor of the carpal tunnel (Fig. 1-16).
Compared to the carpal tunnel syndrome, ulnar tunnel syndrome is less common because the space within the Guyon’s canal is much more yielding. Compression within the canal can produce motor or sensory or combined motor and sensory symptoms. The Guyon’s canal can be divided in three zones to allow more accurate localization of the pathology of the compression in respect to the neurological symptoms (4).
Zone I is the most proximal and is bounded palmarly and radially by the volar carpal ligament, medially by the FCU and the pisiform, and dorsally by the transverse carpal ligament. This region includes both the sensory and the motor branches of the ulnar nerve; therefore, compression in the region results in combined motor and sensory deficits. Compressions within this region are usually produced by fractures of the hook of the hamate and ganglions (Fig. 1-17).
 FIGURE 1-16 The deep motor branch of the ulnar nerve passes under the fibrous arch of the hypothenar muscles ulnar to the hook of the hamate. (P, pisiform; M, motor branch; SPA, ulnar branch to superficial palmar arch; FA, fibrous arch of the hypothenar muscles; S, one of the sensory branches of the ulnar nerve.) |
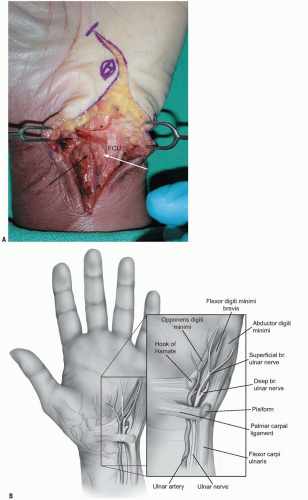 FIGURE 1-17 A,B: Zone I of the ulnar tunnel as described by Gross and Gelberman (asterisk). Note the neurovascular bundle passing under the proximal edge of the palmar carpal ligament. (FCU, flexor carpi ulnaris; white arrow, ulnar artery; black arrow, ulnar nerve.) |
Zone II is bounded palmarly by the palmaris brevis muscle and the fibrous arch of the hypothenar muscles; dorsally by the pisiform and hamate ligaments and the oppenens digiti minimi; medially by the superficial branch of the ulnar nerve and the abductor digiti minimi; and laterally by the transverse carpal ligament, flexor digiti minimi, and the hook of the hamate. This region surrounds the motor branch of the ulnar nerve and compression within this region results in motor symptoms. Ganglions and fractures of the hook of the hamate can produce compression within this region, as well as anomalous intrinsic muscles within the canal (Figs. 1-18 and 1-19).
Zone III is bounded palmarly by the ulnar artery and the palmaris brevis muscle, dorsally by the hypothenar fascia, laterally by the motor branch of the ulnar nerve, and medially by the abductor digiti minimi muscle. This region surrounds the superficial branches of the ulnar nerve, and compression within this region produces exclusively sensory symptoms (Fig. 1-19). The most frequent causes of compression within this region are synovial inflammation, vascular lesions of the ulnar artery (thrombosis, aneurysm, or pseudoaneurysm), and anomalous size and location of abductor digiti minimi.
 FIGURE 1-18 Demonstrates the entrance to zone II of the ulnar tunnel in which the nerve passes under the palmar brevis muscle providing innervation to the muscle (asterisk). (White arrow, ulnar artery; black arrow, ulnar nerve.) |
 FIGURE 1-19 The ulnar nerve passes over the pisohamate and pisometacarpal ligaments which form the floor of the tunnel. Note the branches which supply the hypothenar muscles. The asterisk marks the nerve bifurcation into the deep motor branch (M) and the superficial sensory branches. (P, pisiform; FCU: flexor carpi ulnaris; white arrow, ulnar artery; black arrow, ulnar nerve; SPA, ulnar branch to superficial palmar arch; S RF, sensory branch to ulnar side of ring finger and radial side of the small finger; S SF, sensory branch to the ulnar surface of the small finger; M PB, motor branches to the palmaris brevis muscle.) |
PART 3. Surgical Approaches of Flexor Tendons in Wrist and Hand
David Ruch
Nikolaos P. Zagoreos
The versatility of the human hand depends, to a great extent, on the normal function of the flexor tendons. These collagenous structures are able to transmit enormous forces from the muscles in the forearm to the fingers allowing not only powerful motions but also fine motor activities.
Unfortunately, tendon lacerations are quite common and require prompt tendon surgery and accurate surgical approach. The same approaches can be used to address clinical conditions affecting neighboring structures like the nerves, the vessels, or the bones in the hand.
The various surgical approaches needed for flexor tendon surgery will be presented, as well as brief description of the anatomy of the flexor tendons and of the special properties and considerations of the volar skin of the palm and the fingers.
GROSS ANATOMY OF FLEXOR TENDONS OF THE WRIST AND THE HAND
The flexor muscles originate in the proximal two-thirds and provide the respective flexor tendons in the distal third of the volar compartment of the forearm. Three flexor tendons insert around the area of the wrist; the flexor carpi radialis located on the radial side of the forearm inserts at the base of the second metacarpal; the FCU located in the ulnar aspect of the forearm inserts at the pisiform bone; the palmaris longus located in the most superficial layers along the midline of the forearm inserts at the palmar fascia of the hand. The palmaris longus is absent unilaterally or bilaterally in 12% and is useful in grafting because it is readily accessible and expandable.
The remaining nine flexor tendons are the flexor tendons of the fingers and the thumb; two for each of the fingers and one long flexor for the thumb. They all enter the hand through the carpal tunnel and diverge towards the respective digit where they insert.
There are two flexor tendons for each finger, the flexor digitorum superficialis (FDS) and the flexor digitorum profundus (FDP). The FDS tendons lie more anterior to the FDP within the forearm and the palm and are grouped in two layers within the carpal tunnel. The tendons of the middle and ring fingers lie volarly to those of the index and small fingers. At the palm all the tendons of the FDS lie in the same plane, volar to the tendons of the FDP.
The tendons of the FPD are all in the same plane and are usually not so distinct at the level of the palm with the exception of the tendon to the index. They become more distinct distal to the carpal tunnel. An important anatomical relationship helpful in distinguishing the tendons of the FDP from the FDS in multiple tendon lacerations within the palm is that the four lumbrical muscles take their origin from the tendons of the FDP.
At the level of the metacarpophalangeal joint, the FDS splits into bands. The FDP passes between these two bands becoming more superficial to the FDS forming the Camper’s chiasm. The two bands of the FDS rotate away from the midline so that the most medial fibers become the most volar ones and the most lateral ones become the most dorsal, and insert at the two lateral edges of the base of the middle phalanx. The FDP continues more distally and inserts at the base of the distal phalanx.
The thumb has only one flexor tendon, the flexor pollicis longus (FPL), which enters the carpal tunnel in its most radial aspect. Following the carpal tunnel, the tendon courses around the scaphoid, beneath the thenar musculature, and inserts at the base of the distal phalanx of the thumb.
The tendons of the FDS and FDP for each finger enter a well-defined fibro-osseous tunnel just proximal to the respective metacarpophalangeal joint of the finger. This digital fibrous sheath consists of thick fibrous bands in oblique or transverse orientation, known as pulleys, which keep the tendons close to the phalanges and prevent bowstringing during flexion of the finger. The current nomenclature for the pulley system was established by Doyle and Blythe (1,2), who described five annular “A” (A1-A5) and three cruciate “C” (C1-C3) pulleys. A1, A3 and A5 are located over the metcarpophalangeal, proximal interphalangeal, and distal interphalangeal respectively. A2 and A4 are located over the middle part of the proximal and distal phalanx respectively. The C1 pulley is over the distal end of the proximal phalanx, the C2 pulley over the proximal end of the middle phalanx, and the C3 pulley over the distal end of the middle phalanx (Fig. 1-20).
 FIGURE 1-20 The fibro-osseous tunnel of each finger with the annular A1-A5 and cruciate C1-C3 pulleys. |
The thumb has a similar fibro-osseous tunnel with an annular A1 pulley over the metacarpophalangeal joint, an oblique annular ligament extending from proximal ulnar to distal radial direction over the proximal phalanx of the thumb, and an annular A2 pulley over the interphalangeal joint.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


