CHAPTER 1 Gross Anatomy of the Ankle Joint
The first attempts of arthroscopic interventions were made in the beginning of the 20th century.1 Originally, the knee joint was the focus of attention because of its more accessible anatomy than other joints, such as the ankle, shoulder, and smaller joints. Technical difficulties and the lack of appropriate equipment contributed to the late emergence of ankle arthroscopy compared with other joints.
In the late 1970s, Watanabe and subsequently some of his followers reported on the first attempts of ankle arthroscopy.2 Later, Ferkel, Guhl, and others reported series of ankle arthroscopies, outlining the indications, the type of pathology that could be treated, and long-term outcomes.3–5 They also reported a methodology to evaluate and address the ankle joint from an arthroscopic approach.
TOPOGRAPHIC ANATOMY
Anterior Ankle Topographic Anatomy
The anteromedial aspect of the ankle joint presents the most superficial portion of the distal tibia and the medial malleolus, whose tip is approximately 1 cm distal to the joint line. Slightly anterior to the medial malleolus are the saphenous nerve and the saphenous vein, both of which are located medial to the anterior tibialis tendon. The saphenous vein is at risk for being punctured during the creation of the anteromedial portal (Fig. 1-1).3
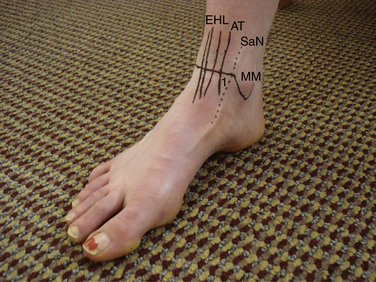
The anterior tibialis tendon represents the lateral margin of the so-called soft spot of the ankle joint. The soft spot is delineated by the anterior tibialis tendon laterally, the most distal portion of the tibial plafond superiorly, and the lateral margin of the medial malleolus medially. This soft spot is the site of choice for placement of the anteromedial portal and for performing intra-articular injections of the ankle joint. The distal medial aspect of the tibia demonstrates a superiorly oriented notch of variable height known as the notch of Harty. This notch often affords easier initial placement of the arthroscopic cannula into the joint. In both applications, penetration of the ankle joint through the soft spot should be as lateral as possible and close to the anterior tibialis tendon to avoid damage to the saphenous vein and possibly to the more medially located saphenous nerve. Portal placement immediately adjacent to the medial border of the tibialis anterior tendon and as far away from the medial malleolus as possible facilitates manipulation of the arthroscope and instruments, avoiding mechanical impingement of the cannula on the medial malleolus.
The extensor digitorum longus (EDL) tendon is located lateral to the anterior neurovascular bundle. Lateral to it, the dorsal cutaneous branch of the superficial peroneal nerve is found, which can be visualized or palpated in most patients by placing the foot in forced maximum plantar flexion and adding maximal plantar flexion of fourth metatarsophalangeal (MTP) joint.6 At the level of the ankle joint line, the course of the dorsal cutaneous branch of the superficial peroneal nerve ranges from the anterior margin of the lateral malleolus to the lateral aspect of the extensor digitorum longus tendon (Fig. 1-2).7
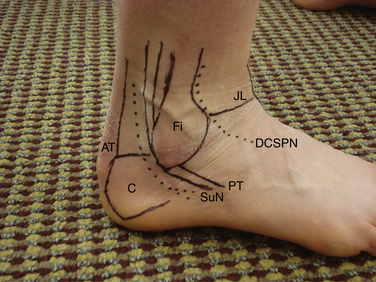
Creation of the anterolateral portal should take the location of the dorsal cutaneous branch of the superficial peroneal nerve into consideration to avoid damage to the nerve. The dorsal cutaneous branch of the superficial peroneal nerve is the neurologic structure at highest risk for complication during ankle arthroscopy.4 It is important to avoid injury to the superficial peroneal nerve by using proper portal creation technique, known as the nick and spread technique. First, only the skin is incised. The knife blade is not allowed to penetrate into the subcutaneous tissues. Second, the subcutaneous tissues are bluntly dissected using a small mosquito forceps. Third, the portal is created using a blunt trocar. The joint capsule is quite thin, and avoiding sharp trocars helps to minimize the likelihood of nerve injury.
Posterior Ankle Topographic Anatomy
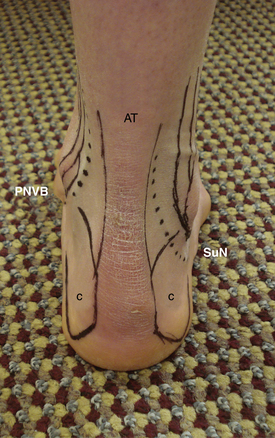
The sural nerve is located between the peroneal tendons and the Achilles tendon, approximately 1 to 1.5 cm distal to the tip of the fibula and 1.5 to 2 cm posterior to it.5 The location of the sural nerve has some variability within the posterolateral aspect of the ankle joint. It is always located close to the lesser saphenous vein.8 These two structures are the only ones at risk in the posterolateral aspect of the ankle joint (Fig. 1-3).
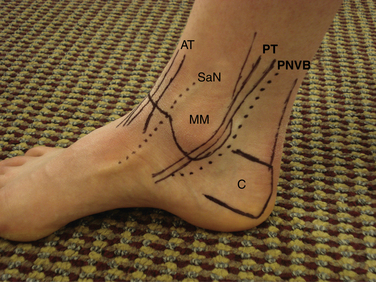
The Achilles tendon has an average width of 1 to 1.5 cm immediately above the superior margin of the calcaneus tuberosity. The deep flexor tendons are located medial to the Achilles tendon, and the flexor hallucis longus (FHL) tendon is the most lateral of the deep flexor tendons. Identification of this tendon is key to avoiding damage to the posterior neurovascular structures. The posterior neurovascular bundle is located immediately adjacent and medial to the FHL, and it includes the posterior tibial artery, veins, and tibial nerve. The flexor digitorum longus (FDL) tendon is located medial to the posterior neurovascular bundle. The posterior tibialis tendon is anterior and medial to the FDL. The posterior tibialis tendon is located on the medial malleolus at the level of the joint line (Fig. 1-4).
INTRA-ARTICULAR ANATOMY AND ACCESS
Related posts:
 Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Instrumentation and Operative Setup for Ankle and Subtalar Arthroscopy
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Instrumentation and Operative Setup for Ankle and Subtalar Arthroscopy
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


