Genu Recurvatum in Total Knee Arthroplasty
Trevor R. Pickering
John B. Meding
E. Michael Keating
INDICATIONS
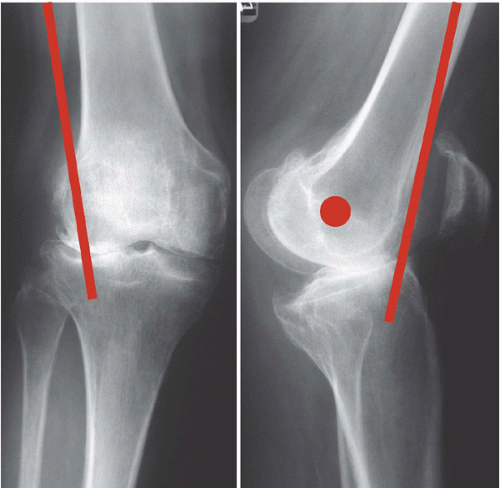
A recurvatum deformity in patients prior to total knee arthroplasty (TKA) is relatively rare and has received little attention in the literature (1, 2, 3, 4, 5, 6). Hyperextension deformities greater than 5 degrees occur in only 0.5% to 1% of TKA candidates (2,5). Because satisfactory postoperative function may be difficult in patients with neuromuscular disorders, the primary goal when determining the appropriateness of TKA in a patient with genu recurvatum is to identify the etiology of the patient’s deformity. If the etiology does not affect the patient’s quadriceps function, the surgeon can proceed with performing TKA. A contracture of the iliotibial (IT) band can result in recurvatum in knees with a fixed valgus deformity (Fig. 11-1) (6). The IT band is anterior to the axis of rotation of the knee when the knee is in extension. In the absence of a knee flexion contracture, an IT band contracture can cause hyperextension. At the time of surgery, erosions will be found on the anterolateral aspect of the tibial plateau (Fig. 11-2). Patients with rheumatoid arthritis can present with significant ligamentous laxity about the knee, which, in turn, can lead to a hyperextension deformity as well (7). Finally, anterior sloping of the tibial plateau, which may be found secondary to trauma or in patients who have undergone a high tibial osteotomy, can predispose to genu recurvatum. In such cases, there is no neuromuscular compromise, and TKA is indicated in the setting of degenerative disease of the knee.
CONTRAINDICATIONS
Recurvatum in individuals with a neuromuscular disorder, as may be seen with poliomyelitis, for example, is common. The outcome of TKA in these patients is generally poor secondary to bone deformity and quadriceps degeneration or paralysis (4,8). In these patients, TKA is generally contraindicated because of the high rate of recurring hyperextension and knee instability after surgery (8).
PREOPERATIVE PREPARATION
Preoperative full-length standing anteroposterior and lateral non-weight-bearing radiographs should be obtained. This provides a preliminary evaluation of coronal and sagittal plane deformities as well as evaluation of the knee’s joint space. A measurement of the recurvatum deformity in the clinic using a goniometer with the patient in a supine position will further characterize its severity. Most importantly, any patient with genu recurvatum who presents for TKA evaluation must undergo a complete assessment of quadriceps, hamstring, and gastrocnemius complex strength and function. Paralysis or significant weakness of the quadriceps may lead a patient to lock the knee in
hyperextension to ambulate. If such locking is inhibited with a knee replacement, these individuals can lose the ability to ambulate completely. Also important is the functional position of the foot and ankle. A plantar flexion contracture of the ankle and weak dorsiflexors will predispose the knee to hyperextension, especially at heel strike and should be corrected before surgery (Fig. 11-3).
hyperextension to ambulate. If such locking is inhibited with a knee replacement, these individuals can lose the ability to ambulate completely. Also important is the functional position of the foot and ankle. A plantar flexion contracture of the ankle and weak dorsiflexors will predispose the knee to hyperextension, especially at heel strike and should be corrected before surgery (Fig. 11-3).