Chapter 14 General Principles of Amputations
Incidence and Indications
Trauma
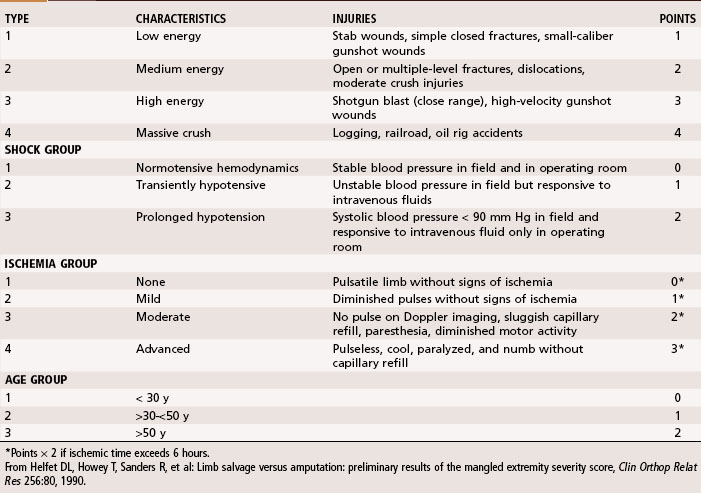
Other authors have attempted to remove subjectivity from the decision-making process. To predict which limbs will be salvageable, available scoring systems include the predictive salvage index, the limb injury score, the limb salvage index, the mangled extremity syndrome index, and the mangled extremity severity score. Of these, we have found the mangled extremity severity score to be most useful (Table 14-1). This system, which is easy to apply, grades the injury on the basis of the energy that caused the injury, limb ischemia, shock, and the patient’s age. The system was subjected to retrospective and prospective studies, with a score of 6 or less consistent with a salvageable limb. With a score of 7 or greater, amputation was the eventual result. Although we do not strictly follow these guidelines in all patients, we do calculate and document a mangled extremity severity score in the chart whenever we are considering primary amputation versus a complicated limb salvage.
Infection
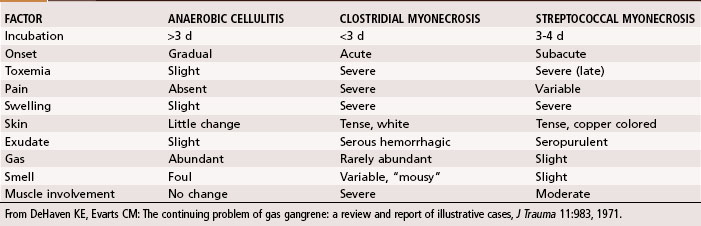
Three distinct gas-forming infections must be differentiated (Table 14-2). The first is clostridial myonecrosis, which typically develops within 24 hours of closure of a deep contaminated wound. The patient has an acute onset of pain, swelling, and toxemia, often associated with a mental awareness of impending death. The wound develops a bronze discoloration with a serosanguineous exudate and a musty odor. Gram stain of the exudates shows gram-positive rods occasionally accompanied by other flora. Treatment consists of immediate radical débridement of involved tissue, high doses of intravenous penicillin (clindamycin may be used if the patient is allergic to penicillin), and hyperbaric oxygen. Emergency open amputation one joint above the affected compartments often is needed as a lifesaving measure but may be avoided if treatment is initiated early.
Tumors
1. Would survival be affected by the treatment choice?
2. How do short-term and long-term morbidity compare?
3. How would the function of a salvaged limb compare with that of a prosthesis?
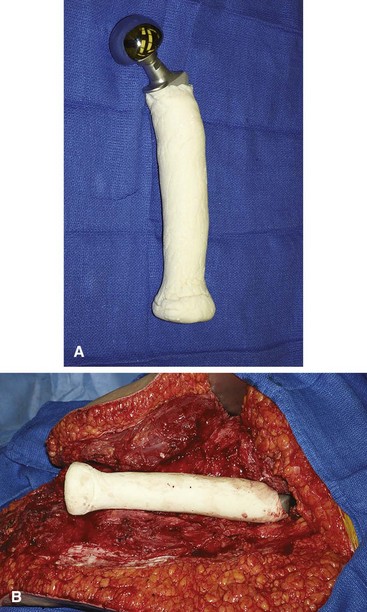
Amputation for malignancy may be technically demanding, often requiring nonstandard flaps, bone graft, or prosthetic augmentation to obtain a more functional residual limb (Fig. 14-1). Limb salvage is associated with greater perioperative morbidity, however, compared with amputation. Limb salvage involves a more extensive surgical procedure and is associated with greater risk of infection, wound dehiscence, flap necrosis, blood loss, and deep venous thrombosis. Long-term complications vary depending on the type of reconstruction. These include periprosthetic fractures, prosthetic loosening or dislocation, nonunion of the graft-host junction, allograft fracture, leg-length discrepancy, and late infection. A patient with a salvaged limb is more likely to need multiple subsequent operations for treatment of complications. After initial successful limb salvage surgery, one third of long-term survivors ultimately may require an amputation.