84
Ganglions
Kevin D. Plancher and Michael Bothwell
History and Clinical Presentation
A 38-year-old woman presents with a painful mass on her wrist. The patient complains about the size of this mass, and the continued disappearance and recurrence of the mass. The mass enlarges and is more painful after activity. The patient reports no history of a puncture wound or other trauma. There is no previous history of arthritis. The patient has had no previous treatment of the mass.
Physical Examination
A firm mass on the dorsum of the wrist is palpated (Fig. 84–1). The mass is smooth, fluctuant, and round; it is located over the mid-dorsal carpal area, and originates from the scapholunate ligament. Palmar wrist flexion accentuates the size and shape of the mass. Vascular examination entails palpation of pulses, and Allen’s test to rule out arterial compromise. Gentle percussion of the lesion did not elicit Tinel’s sign, ruling out peripheral nerve encroachment. Using a small light, the lesion was transilluminated. The passage of light through the mass confirms the diagnosis of a cystic type lesion and helps define the boundaries of the lesion.
Diagnostic Studies
Radiographs verify the location, identified by a soft tissue shadow. Radiographs are also used to assess associated pathologies including arthritis or carpal instability. If the diagnosis or the boundaries are unclear, ultrasound and magnetic resonance imaging (MRI) are useful studies.
Differential Diagnosis
Inclusion cysts
Synovitis
Tenosynovitis
Rheumatoid nodules
Lipomas
Carpal bosses
Osteochondromas

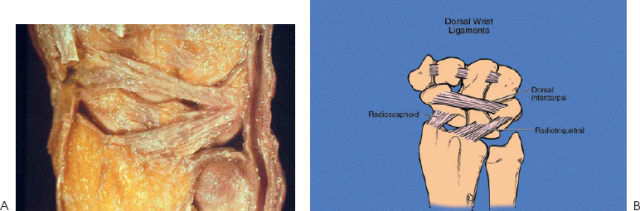
Figure 84–1. Typical clinical appearance of dorsal carpal ganglion.
Diagnosis
Dorsal Wrist Ganglion
Sixty to seventy percent of wrist ganglions are found on the dorsal surface. They rarely exceed 2 cm in diameter and are almost always found between the dorsal intercarpal ligament and radiotriquetral ligament, centered over the scapholunate ligament (Fig. 84–2).
Ganglions are benign cystic lesions that contain a mucinous, viscous fluid. They are the most common benign soft tissue tumor of the upper extremity. These tumors are more common in women than in men and usually occur in the second through fourth decades. Ganglions have a smooth, whitish, fibrous wall of variable thickness filled with jelly-like mucous, containing glucosamine, albumin, globulin, and hyaluronic acid. The cyst’s neck narrows to a stalk and is usually connected to fibrous ligaments tissue.
Several etiologies have been proposed to explain their presence. The theories include cystic formation secondary to mucoid degeneration of connective tissue; synovial herniation from a joint; cysts that arise from the wrist capsule, which attaches to the scapholunate interosseous ligament and when stressed acts as a synovial fluid pump; and ganglions that arise secondary to a traumatic event. Ganglions can be dorsal, occult, or volar in the hand or wrist.
Surgical Management
Surgical treatment of a dorsal carpal ganglion should be performed with general or regional anesthesia. Higher recurrence rates have been noted with the use of local anesthesia. A transverse incision is made over the proximal third of the ganglion. The dorsal cutaneous branch of the radial nerve should be protected. The extensor retinaculum over the ganglion is excised, and the extensor carpi radialis longus and brevis are isolated and retracted radialward. The extensor digitorum communis to the index finger is then retracted with the remaining extensor tendons ulnarward. The mass is identified and mobilized in a circumferential fashion. Surgical treatment should focus on removing the ganglion cyst and all material between the radiotriquetral ligament and dorsal intercarpal ligament. The ganglion is excised with all of its attachments to the joint capsule and scapholunate ligament (Fig. 84–3). Capsular closure is not recommended. The lesion should be inspected on the back surgical table to verify diagnosis and sent to pathology for definitive histologic analysis. The wound is irrigated, hemostasis is obtained, and the skin is closed.