Although there is a great deal of published material on fractures of the shoulder girdle in the historical literature, these are relatively uncommon overhead sporting injuries. In the nonathletic population, fractures of the shoulder girdle are historically most common in the early adolescent patient who has open physes and in the older patient who has osteoporosis. In most active young and middle-aged overhead athletes, the bony structures of the shoulder appear to be less vulnerable to injury than the soft tissue structures (glenohumeral ligaments, labrum, and rotator cuff) about the shoulder. Shoulder instability and rotator cuff injury, therefore, are far more common than fractures in overhead athletes. However, high-energy direct or indirect trauma can cause fractures of the humerus, clavicle, or scapula.
Fractures of the shoulder girdle can lead to significant morbidity in the overhead athlete and require aggressive treatment to return to competitive sport. Precise anatomic reconstruction is often necessary to restore the shoulder to its normal biomechanical abilities. Precise diagnosis of fracture type and configuration is essential for accurate treatment. The judicious use of open reduction and internal fixation techniques has become an integral part of the treatment program to achieve anatomic restoration of the shoulder. Equally important is an early aggressive rehabilitation program designed to prevent the common problems of residual stiffness and dysfunction that can compromise the treatment of these fractures.
ANATOMY AND BIOMECHANICS
Proximal Humerus Anatomy and Biomechanics
The shoulder is the most mobile major joint in the body. The primary function is to position the hand in space to accomplish prehensile activity. The anatomic features of the proximal humerus and glenohumeral joint are well suited to provide this function. The proximal humerus consists of four well-defined parts that include the humeral head, the lesser and greater tuberosities, and the proximal humeral shaft. The proximal humerus arises from three distinct ossification centers, including one for the humeral head and one each for the lesser and greater tuberosities. The fusion of the ossification centers creates a weakened area in the construct, known as the epiphyseal scar, making these regions of the proximal humerus susceptible to fracture. The articular surface of the humeral head is two to three times larger than the surface area of the glenoid. The relatively flat glenoid produces very little constraint to humeral motion. The range of motion of the glenohumeral joint is 2:1 that of scapulothoracic motion, and their combined motion approximates to 180 degrees of abduction. The humeral neck shaft angle is approximately 45 degrees, and the head is 30 to 40 degrees retroverted relative to the epicondyles at the elbow. The anatomic configuration aligns the humeral head with the scapula as it lies along the posterolateral thorax in the anatomic plane.
The synergy between the stabilizing effect of the rotator cuff and the biceps combined with the power of the deltoid provides normal dynamic shoulder function. The deltoid is the primary motor source for the shoulder but also creates a shear stress across the joint. The rotator cuff and biceps provide stability by counterbalancing the humeral head against the deltoid shear. As internal rotation and external rotation components are added, the rotator cuff muscles provide not only humeral head depression but also stability against excessive anterior and posterior translation within the joint. Fractures of the shoulder girdle that disrupt or distort this finely tuned anatomy can alter the biomechanics of the shoulder and therefore lead to limitation of motion and function. Restoration of the anatomy along with appropriate muscle strength and coordination are necessary to return the shoulder to normal function.
Disruption of the arterial blood supply to the proximal humerus from trauma or surgical intervention can result in avascular necrosis of the humeral head. There are three main arterial contributions to the proximal humerus (1,2). The major arterial contribution to the humeral head segment is the anterior humeral circumflex artery. The terminal portion of this vessel, the arcuate artery, is interosseous in nature and perfuses the entire epiphysis. If this vessel is injured, only an anastomosis distal to the lesion can compensate for the resulting blood loss. Less significant blood supply to the proximal humerus is delivered by a branch of the posterior humeral circumflex artery, as well as the small vessels entering through the rotator cuff insertions. The posterior humeral circumflex artery, which penetrates the posteromedial cortex of the humeral head, is thought to supply only a small portion of the posteroinferior part of the articular surface of the humerus compared with the arcuate artery. The vessels that enter the epiphysis via the rotator cuff insertions are also thought to be inconsequential as well as inconsistent in their vascular supply to the humeral head.
The local nerve anatomy about the shoulder is comprised of the brachial plexus, which lies anterior to the scapula, passing below the coracoid to enter the upper arm. The axillary nerve arises from the posterior cord and courses first along the anterior surface of the subscapularis muscle belly and then below the glenohumeral joint to innervate the deltoid and teres minor. The musculocutaneous nerve arises from the lateral cord, penetrating the coracobrachialis muscle 5 to 7 cm distal to the coracoid (3). The brachial plexus therefore is tethered in its position anteromedial to the proximal humerus and is vulnerable to injury in displaced fractures. The axillary nerve is most frequently injured portion of the plexus in proximal humerus fractures.
Clavicle Anatomy and Biomechanics
The embryologic development of the clavicle occurs through a combination of intramembranous and endochondral ossification. The central portion is the first area of ossification and is responsible for the growth of the clavicle up until the age of 5 years (4,5). Medial and lateral epiphyseal growth plates eventually develop, with only the sternal ossification center being visible radiographically (4). The medial clavicular epiphysis is the most important to longitudinal growth and contributes as much as 80% of the entire length (6). The physis fuses between the ages of 22 and 25 years.
The clavicle is the only bone that connects the trunk to the shoulder girdle. It is attached medially to the sternum and laterally to the scapula by a combination of extraarticular and capsular ligaments. The bony architecture is not only important to its function but also to providing an explanation for the pattern of fractures encountered. The clavicle has a double S-shaped curve that varies in cross-sectional area along its length. The medial portion is tubular and resists axial loading. This portion of the clavicle protects the costoclavicular space, where the medial cord and origin of the ulnar nerve are at risk for injury with medial clavicle fractures, clavicular nonunions, and healed fractures with exuberant callus. The flat lateral portion functions to resist the muscular and ligament forces. The weakened junction of the medial tubular and flattened lateral clavicle places the middle clavicle at risk for fracture (7).
It is important to understand the relationship of the soft tissue structures to the clavicle. This knowledge lessens the risk of damage to vital structures during treatment. The clavicle is a bony framework for muscle origins and insertions. The soft tissue structures that surround the bony clavicle can be divided into the areas above, below, and behind this structure. Above the clavicle, the cervical fascia, sternocleidomastoid muscle, omohyoid, and upper third of the trapezius insert from medial to lateral onto the superior aspect of the clavicle. Below the clavicle, the clavicular head of the pectoralis major and minor attaches medially while the anterior deltoid is attached laterally. Finally, behind the clavicle, although no muscles directly insert, there is a continuous myofascial layer that lies in front of the large vessels and nerves as they pass from the root of the neck to the axilla. Behind the medial clavicle, the internal jugular and subclavian veins join to form the innominate vein. Behind the midportion are both the subclavian and axillary veins.
ETIOLOGY OF INJURY
The most common mechanism of fracture to the athletic shoulder girdle is a fall on an outstretched arm, as commonly occurs in both contact and noncontact sports. In athletic patients, significant trauma is necessary, and the resultant fracture is often more serious than those that occur in older patients with osteoporotic fractures. These younger patients commonly have displaced fractures or fracture-dislocations with substantial soft tissue disruption. Neurologic or vascular injury can occur and are related to the seriousness of the soft tissue component of the injury.
An additional mechanism of fracture of the proximal humerus occurs with excessive external rotation of the arm. The proximal humerus is wedged against the acromion in a pivotal position, and a proximal humerus fracture can occur through this area. A direct blow to the lateral arm can also cause injury to the shoulder girdle. The mechanism usually results in a fracture of the greater tuberosity, a minimally displaced fracture, or a fracture involving the articular surface. Fractures associated with primary dislocation of the shoulder, both anterior and posterior, are usually caused by the forced abducted, externally rotated position (for anterior fracture-dislocation) and forced adduction with posterior displacement (for posterior fracture-dislocation).
Clavicular fractures may result from direct or indirect trauma. Patients involved in stick sports such as lacrosse and hockey frequently sustain a direct blow to the clavicle. In addition, a fall directly onto the bone itself can result in a fracture. Clavicular injuries may also occur from a fall onto the outstretched arm, but this is probably a less common mechanism of injury. Medial clavicle fractures are most common secondary to indirect trauma from a force directed to the lateral arm.
Although the most common cause of humeral fractures is blunt trauma, a spiral fracture of the shaft of the humerus resulting from muscular violence has been reported in various overhead throwing sports, including baseball, javelin, and handball, as well as in arm wrestling. This has become a well-recognized clinical entity. Many explanations for the spiral fracture have been offered, most being variations of torsional stress injury. Powerful internal rotation is applied to the upper shaft of the humerus by the pectoralis major, subscapularis, teres major, and latissimus dorsi while a force across the forearm imparts external rotation to the distal humerus through the elbow joint.
PRESENTATION AND PHYSICAL EXAMINATION
Athletes who sustain fractures of the shoulder girdle typically describe specific trauma and can often attribute the mechanism of injury. After the fracture pain, swelling and inability to use the shoulder are seen immediately. Most patients are not able to continue to participate in the athletic activity.
A meticulous evaluation of the injured shoulder girdle begins with a visual examination by adequately exposing the shoulder girdle and upper extremity. Deformity is more common with dislocations and displaced fractures about the shoulder. Fracture-dislocations may be less apparent than true dislocations, in that the arm may hang in a more normal position at the side. In proximal humerus fractures, the deltoid and soft tissue may mask significant fracture displacement or dislocation. By 48 hours after injury, ecchymosis may extend down the chest wall or to the elbow. Posterior sternoclavicular fracture dislocations and posteriorly displaced lateral clavicle fractures can frequently be missed without a careful examination.
Other areas are evaluated in addition to obvious shoulder girdle fractures. The cervical spine is assessed for any tenderness and pain with motion. If there is any question, cervical spine radiographs are obtained before any movement of this area. Direct tenderness over a fresh or healing fracture has always been a useful clinical sign for the ribs, clavicle, acromion, and humerus and often indicates the area of concern. Pain or tenderness may be elicited indirectly with motion or with longitudinal compression or distraction.
Neurologic evaluation is carried out for all components of the upper extremity. Gentle motion and isometric contractions are generally sufficient to allow palpation of individual muscle groups as a screening test for muscle integrity and nerve supply. In the distal part of the involved limb, the color, capillary refill, and radial pulse are examined and compared with those of the uninjured upper extremity. More detailed vascular evaluation is undertaken if arterial injury is suspected.
RADIOGRAPHIC AND DIAGNOSTIC EVALUATION
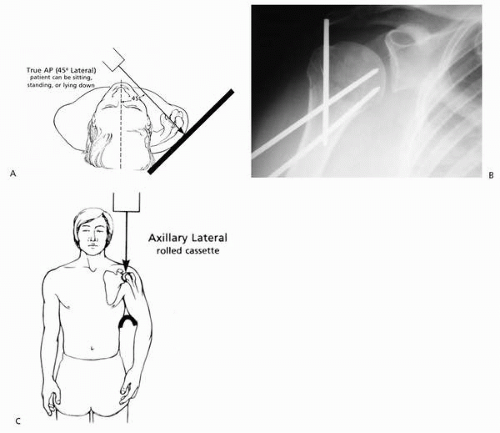
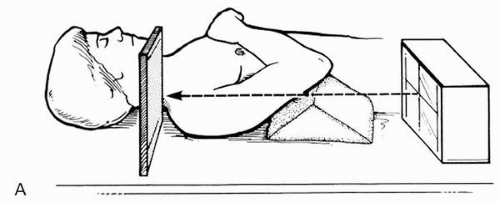
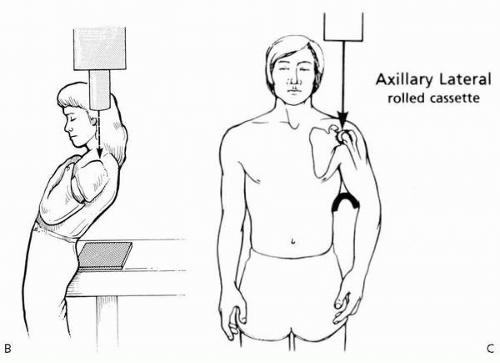
The radiologic evaluation of proximal humerus fractures begins with plain radiographs. The trauma shoulder series involves three views: a true anteroposterior (AP) view of the shoulder in the plane of the scapula with the arm in internal and external rotation and an axillary lateral or a scapulolateral view (Fig. 18-1). The axillary view is a valuable view in the evaluation of the proximal humerus fracture and must not be neglected. Radiology technicians are often reluctant to position the shoulder for an axillary view due to the significant pain that the patient feels with even the slightest motion. When a supine axillary view cannot be obtained, an alternative axillary view should be obtained. These include a trauma axillary lateral view, a Velpeau axillary lateral view, or an axillary view with flexible radiographic (mammography) film (Fig. 18-2). Alternatively, a transthoracic lateral view may be helpful if the scapulolateral view (scapular Y view) or other axillary views are difficult to obtain.
When the degree of displacement of the humeral head or tuberosity fragments is uncertain, then an axial computed tomography (CT) study with 2-mm sections is indicated. CT also assists in analyzing the size of humeral head impression fractures, the extent of articular involvement in head-splitting fractures, and the displacement or extent of comminution of associated glenoid fractures. Three-dimensional reconstruction views are not routinely indicated, but may help in the preoperative planning of complex, comminuted fractures or complex malunions.
The most beneficial screening examination for clavicle fractures is the anteroposterior (AP) view. When this view is obtained, the films should include the upper third of the humerus, the shoulder girdle, and upper lung fields so that other girdle fractures or a pneumothorax can be quickly identified. When a high-energy injury occurs, a chest x-ray study should be obtained to evaluate for a pneumothorax or rib fractures. The configuration of the fracture may suggest other associated injuries. For lateral clavicle fractures, a 15-degree cephalic tilt radiograph should always be obtained to evaluate the lateral articular segment and acromioclavicular joint.
FIGURE 18-1. Trauma shoulder series. Recommended views for the evaluation of proximal humerus fractures include a true anteroposterior view in the plane of the scapula with the arm in internal and external rotation (A) and an axillary lateral (B) or scapulolateral view (C). (From Rockwood CA, Jensen KL. X-ray evaluation of shoulder problems. In: Rockwood CA, Matsen FA, eds. The shoulder, vol. 1, 2nd ed. Philadelphia: WB Saunders, 1998:199-202, with permission.)
FIGURE 18-2. Modified axillary views. If the standard axillary lateral x-ray cannot be obtained, one of the modified axillary views must then be attempted. The trauma axillary lateral x-ray (A) positions the patient supine with the elbow elevated by a piece of foam rubber, allowing the x-ray to pass from the inferior up through the glenohumeral joint onto the x-ray cassette, which is superior to the shoulder. The Velpeau axillary lateral x-ray (B) positions the patient leaning the shoulder backward over a cassette with the beam directed inferiorly. A curved cassette or flexible (mammography) radiographic film can be placed in the axilla and the beam directed inferiorly through the glenohumeral joint onto the cassette. (From Rockwood CA, Jensen KL. X-ray evaluation of shoulder problems. In: Rockwood CA, Matsen FA, eds. The shoulder, vol 1, 2nd ed. Philadelphia: WB Saunders, 1998:202-205, with permission.) Modified axillary views. If the standard axillary lateral x-ray cannot be obtained, one of the modified axillary views must then be attempted. The trauma axillary lateral x-ray (A) positions the patient supine with the elbow elevated by a piece of foam rubber, allowing the x-ray to pass from the inferior up through the glenohumeral joint onto the x-ray cassette, which is superior to the shoulder. The Velpeau axillary lateral x-ray (B) positions the patient leaning the shoulder backward over a cassette with the beam directed inferiorly. A curved cassette or flexible (mammography) radiographic film can be placed in the axilla and the beam directed inferiorly through the glenohumeral joint onto the cassette. (From Rockwood CA, Jensen KL. X-ray evaluation of shoulder problems. In: Rockwood CA, Matsen FA, eds. The shoulder, vol 1, 2nd ed. Philadelphia: WB Saunders, 1998:202-205, with permission.)
FIGURE 18-2.Continued.
CLASSIFICATION OF INJURY
Proximal Humerus Fractures
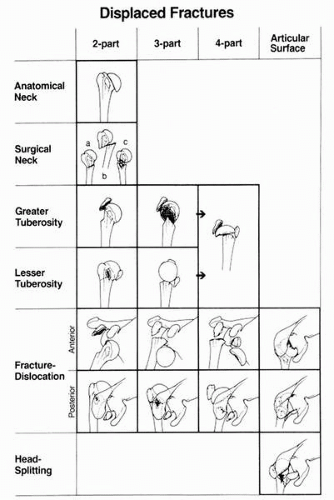
Classification systems of proximal humerus fractures have been designed to offer a common language for discussing these fractures. The two most commonly used systems are the Neer classification and the AO/ASIF classification. The Neer classification was published in 1970 and represents a refinement of Codman’s four-segment classification (i.e., articular segment, greater tuberosity, lesser tuberosity, and humeral shaft) that incorporates the concepts of displacement and vascular isolation of the articular segment (Fig. 18-3) (8,9). The system uses displacement and angulation of the segments to categorize them into one of four groups of fractures: nondisplaced fractures, fractures involving displacement of two fragments, those involving displacement of three fragments, and those involving displacement of all four fragments, with or without dislocation of the articular segment. Specific criteria for determination of a displaced fracture segment was arbitrarily defined by Neer as displacement more than 10 mm or angulation greater than 45 degrees. These values were intended merely as guidelines for differentiating nondisplaced from displaced fracture segments and remain unsubstantiated by experimental or clinical data.
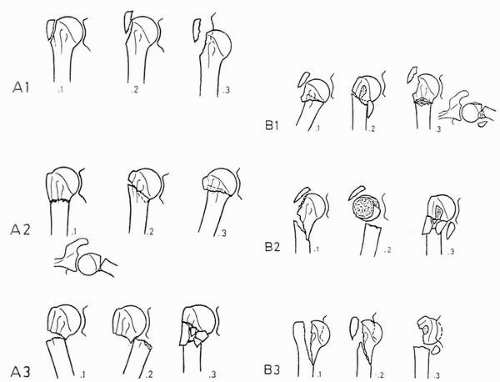
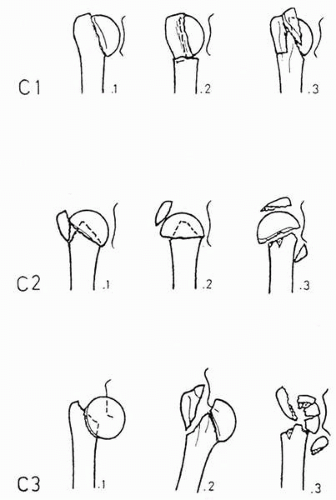
The AO/ASIF group devised a proximal humerus fracture classification in 1987 that included additional subgroupings in an attempt to combine a more detailed analysis of fracture anatomy with the presumed vascular status of the articular segment (10) (Fig. 18-4). The system involves three fracture groups: type A (extraarticular fractures), type B (bifocal fractures; i.e., fracture lines at two locations), and type C (intraarticular fractures). Subgroups are divided into type 1 (nondisplaced/minimally displaced), type 2 (displaced), and type 3 (displaced with comminution/dislocated). This classification provides a more detailed method for fracture description and documentation and a more specific algorithmic approach to treatment.
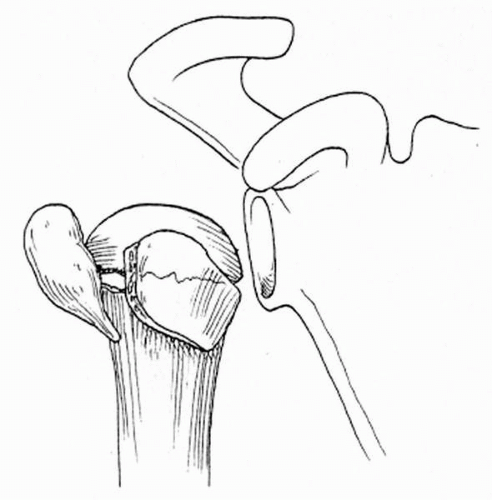
Jakob and colleagues described a distinctive fracture pattern of the proximal humerus in 1991 termed the “valgus-impacted four-part fracture” (11). A valgus-impacted head fragment is the characteristic feature of this fracture pattern (Fig. 18-5). The incidence of osteonecrosis is lower with this fracture type than it is for other displaced four-part proximal humerus fractures. Either closed reduction or limited open reduction and minimal internal fixation led to a 74% satisfactory outcome in their study. The valgus-impacted four-part fracture is suggested to cause less destruction to the proximal humeral blood supply.
Clavicle Fractures
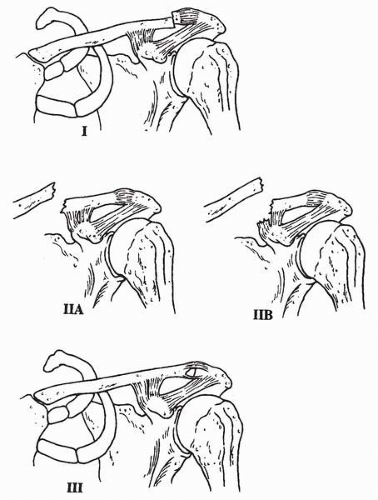
Clavicle fractures are most commonly classified according to location. Although there is not one generally accepted classification scheme, Craig’s classification (12) is useful in understanding fracture anatomy, mechanism of injury, clinical presentation, and alternative methods of treatment. In this classification, three groups exist, depending on the anatomic location of the fracture: distal third, middle third, and inner third fractures. Middle third fractures involve the diaphyseal midshaft portion, comprise 80% of all clavicle fractures, and carry a high union rate. Inner third fractures comprise only 15% of clavicle fractures. Fractures involving the distal third make up the remaining 15% of fractures. Neer recognized the difficulties in treating distal third fractures and proposed a further subdivision into three types (13) (Fig. 18-6). Type I is a distal third fracture with minimal displacement. Type II involves a displaced fracture that occurs at the attachment of the coracoclavicular ligaments to the clavicle. This type is then further subdivided into types IIA and IIB, depending on whether the ligaments remain intact. Type IIA fractures are those in which the coronoid and trapezoid ligaments remain attached to the distal segment. In this case, because the medial fragment has no attached ligaments, it becomes unstable and displaces superiorly as a result of the pull of the sternocleidomastoid muscle. This fracture pattern results in a greater rate of nonunion. A type IIB fracture occurs within the area of the coracoclavicular ligament attachment. In these fractures, the coracoid ligament is disrupted while the trapezoid ligament remains attached to the distal segment. This pattern is more stable than the type IIA fracture. The type III fractures are intraarticular at the acromioclavicular joint.
FIGURE 18-3. The anatomic (Neer) classification of proximal humerus fractures. Each of the four major segments (head, shaft, greater tuberosity, and lesser tuberosity) is considered a fracture part if it is angulated greater than 45 degrees or displaced greater than 1 cm. (From Bigliani LU, Flatow EL, Pollock RG. Fractures of the proximal humerus. In: Rockwood CA, Matsen FA, eds. The shoulder, vol 1, 2nd ed. Philadelphia: WB Saunders, 1998:342.)
FIGURE 18-4. The AO/ASIF classification of proximal humerus fractures. A: Type A fractures. B: Type B fractures. C: Type C fractures. (From Gerber C, Warner JJP. Alternatives to hemiarthroplasty for complex proximal-humeral fractures. In: Warner JJP, Iannotti JP, Gerber C, eds. Complex and revision problems in shoulder surgery. Philadelphia: Lippincott-Raven, 1997:217-218.)
FIGURE 18-4.Continued.
FIGURE 18-5. The four-part valgus impacted fracture of the proximal humerus with an intact medial periosteal bridge. (From Naranja RJ, Iannotti JP. Displaced three- and four-part proximal humerus fractures: evaluation and management. J Am Acad Orthop Surg 2000;8(6):376.)
FIGURE 18-6. Classification of distal clavicle fractures. Type I: The ligaments are intact and there is minimal displacement of the distal clavicle fracture. Type IIA: The fracture is medial to the acromioclavicular ligaments with both ligaments intact. Type IIB: The fracture is between the acromioclavicular ligaments with the conoid ligament disrupted. Type III: Intraarticular fracture of the distal clavicle. (From Schlegel TF, Hawkins RJ. Management of distal clavicle fractures. Oper Tech Sports Med 1997;5(2):94.)
NONOPERATIVE TREATMENT, REHABILITATION, AND RESULTS
Nonoperative care is typically reserved for minimally displaced or nondisplaced fractures of the shoulder girdle. Most shoulder girdle fractures (80% to 85%) belong to this category. Fractures with minimal degrees of displacement and angulation are typically well tolerated functionally even in the throwing athlete. A short period of initial immobilization followed by early motion has been consistently described by most authors as having a high degree of success in treating these fractures.
Most treatment programs stress early motion to prevent the formation of scarring in the capsule, subacromial space, and other surrounding soft tissues that often leads to decreased function. Therapy programs for the nonoperative treatment of shoulder girdle fractures are typically divided into three phases: (a) the passive stretching phase, (b) the active stretching phase, and (c) the strengthening phase. The time frame for individual phases varies between fracture area and configuration (i.e., stable versus unstable). The time frame for each phase can therefore be modified according to the extent of the injury. Specific nonoperative programs for the treatment of clavicle fractures and proximal humerus fractures in the overhead athlete are outlined in Tables 18-1 and 18-2.
TABLE 18-1. NONOPERATIVE SHOULDER CONDITIONING THERAPY FOR CLAVICLE FRACTURES
Phase I: 0-2 weeks
ICE
7 days per week
2-3 times per day after exercising or as necessary
15-20 min “ON” maximum, 60 min “OFF” minimum
STRETCHING: PASSIVE MOTION
7 days per week, 3 times per day
Pendulum exercise: short arc, 1-2 sets, 20-30 repetitions (reps)
Standing internal rotation to belt line (thumb behind back): 1-2 sets, 5-10 reps
Supine-seated forward elevation to 90°, 1-2 sets, 5-10 reps
STATIONARY CYCLING
5 days per week, 1 time per day
Spin or light resistance and increase as tolerated: 10-15-20-30 minutes
Phase II: 2-6 weeks
ICE as per phase I
STRETCHING: ACTIVE MOTION (WITH TERMINAL STRETCH)
7 days per week, 3 times per day
Pendulum exercise: short arc, 1-2 sets, 20-30 reps
Standing internal rotation to belt line (thumb behind back): 1-2 sets, 5-10 reps
Most proximal humerus fractures are nondisplaced and can be managed with conservative care. The periosteum, capsule, and rotator cuff limit fracture displacement so the reduction is unnecessary. The constrained design of the glenohumeral joint and the global range of motion of the shoulder motion provide the advantage that it can compensate for even moderate amounts of residual fracture displacement.
Assisted motion exercises may begin when the fragments move in union. This can be determined by the examiner grasping the humeral head between the thumb and index finger of one hand and rotating the elbow with the opposite hand. The absence of pain, crepitus, and movement between the shaft and the proximal humerus suggests clinical continuity. Once this has been documented, passive range of motion may begin as early as 2 but more often after 3 weeks after the fracture. Overly aggressive activity before this stage may distract the minimally displaced fracture, resulting in either malunion or nonunion of the fracture. Intermittent radiographs are necessary to confirm that there is no displacement of the fracture during healing and physical therapy exercises.
As the fracture becomes more stable, it is then possible to progress therapy to include active exercises with terminal stretch and eventually resisted strengthening exercises. This program should be well designed and carefully monitored and continued until union. Satisfactory functional outcome often takes place between 6 and 12 months.
Clavicle Fractures
Nonoperative treatment is typically recommended for most clavicle fractures. Type I and type III distal clavicle fractures usually require no special treatment and have a favorable outcome with rapid healing after symptomatic care. A sling or figure-of-eight splint is provided for comfort until the pain subsides. Early motion is initiated as tolerated and can begin within days of the injury. Resistive strengthening can begin when the fracture is healed. Recovery is usually rapid and outcome expected to be good. Persistent symptoms occur in a very small percentage of patients. Neer (14) reported that only 2 of 75 patients treated nonoperatively with type I fractures had difficulties. Similarly, Nordquist (15) documented that only 11% of his patients treated nonoperatively went on to have residual problems. There are conflicting results on the long-term complications of type III fractures. Neer found that these often led to AC arthrosis or osteolysis. Nordquist, on the other hand, found no evidence of AC arthritis or distal clavicle osteolysis in his study. If late symptoms develop in either type I or III fractures, then a distal clavicle resection can be performed with good results.
Most fractures of the clavicular shaft can be managed with a well-padded commercial figure-of-eight splint or sling for comfort only. Occasionally, a closed reduction is necessary. A postreduction radiograph is used to evaluate the reduction. Rehabilitation is started as soon as the patient can participate comfortably. It is rare that a fracture of the shaft of the clavicle requires an open reduction and internal fixation. If a completely displaced fracture of the midshaft of the clavicle cannot be reduced with closed manipulation, the patient is observed for 2 to 3 weeks in the figure-of-eight splint. If after observation the complete displacement persists, open reduction and internal fixation can be recommended.
Recent studies have evaluated the sequelae and deficits following conservative treatment of displaced clavicle fractures. Nowak and associates (16) reported that 46% of patients with clavicle fractures demonstrated sequelae (pain during activity, pain at rest, or cosmetic defects) at a 9- to 10-year follow-up. Nonunion occurred in 6% of these patients. No bony contact was the strongest radiographic predictor for sequelae. Comminuted fractures with transversely placed fragments had a significantly increased risk for remaining symptoms, as had older patients. Fracture location and shortening did not predict outcome, except for cosmetic defects. McKee and associates (17) reported on previously unrecognized deficits following conservative treatment of displaced midshaft clavicle fractures and detected residual deficits in shoulder strength, especially endurance. They concluded that the significant level of dissatisfaction following conservative care should encourage more active treatment options in selected patients.
Spiral Humerus Shaft Fractures
The nonsurgical treatment of spiral diaphyseal humeral fractures has long been known to render satisfactory results in most instances. Plate fixation and intramedullary nailing can be associated with a relatively high incidence of complications, such as nonunion, infection, and nerve palsy. Functional bracing of these fractures can offer effective nonoperative management of the majority of these fractures. Indications for functional bracing of humeral shaft fractures include closed diaphyseal fractures without marked distraction between the fragments and closed fractures associated with initial radial nerve palsy. Open fractures without significant soft tissue damage can also be treated with functional bracing following surgical irrigation and debridement and closure of the open wound. Contraindications include bilateral humeral fractures on fractures in polytraumatized patients unless they are able to stand erect early and ambulate with external support on the opposite side.
Functional bracing of humeral shaft fractures begins with stabilization in an above-the-elbow cast or a coaptation splint that holds the elbow in 90 degrees of flexion. A cuff and collar are added for support. On occasion, when the fracture is the result of a low-energy injury and there is minimal swelling of the extremity, the functional brace can be applied at the first encounter. Otherwise, it is best to use a cast or splint until the acute symptoms and swelling subside. In most instances, the brace is applied approximately 12 days after the injury (18, 19, 20).
Pendulum exercises are begun the first postinjury day and are continued after the application of the brace to prevent contracture of the shoulder joint. Active elevation and abduction are avoided. The cuff and collar are discontinued when the elbow reaches full extension but should be used during recumbency for an additional 2 weeks. During ambulation, the arm hangs at the side of the body and swings normally. The brace must be adjusted and fastened with Velcro straps to maintain constant compression of the soft tissues and to prevent displacement of the brace, which is likely to occur as swelling subsides and atrophy develops.
Radiographic evaluation of the fracture should follow the application of the brace and be repeated 1 week later and then at 3- to 4-week intervals. Failure to obtain acceptable alignment of the fragments calls for abandoning the closed treatment and beginning of a different treatment modality. Once the brace is discontinued, there is frequently limitation of motion of the shoulder. However, it improves after return to normal activities. The limitation of shoulder motion ranges from 0 to 15 degrees (18, 19, 20). Limitation of motion at the elbow is less, ranging from 0 to 10 degrees.
Only gold members can continue reading. Log In or Register to continue