Footwear
Foundation for Lower Extremity Orthoses
Jennifer M. Bottomley
Learning objectives
On completion of this chapter, the reader will be able to:
The most essential element of clothing in any person’s wardrobe is the shoe. No other article of clothing is designed to fit so precisely. Continuous pressure from tight shoes can produce ulceration and deformities. Ill-fitting shoes can create shear forces that lead to skin breakdown, create and facilitate toe and foot deformities, and lead to falls.1 Shoes perform the vital functions of transferring body weight to the floor during walking and of protecting the wearer from any hazards in the environment. A well-designed shoe is the necessary foundation for many lower extremity orthotics and for prosthetic alignment and an energy-efficient gait. This chapter discusses the components and characteristics of shoes, ensuring proper fit, and choosing appropriate footwear for patients with foot dysfunction and deformity.
Components of a good shoe
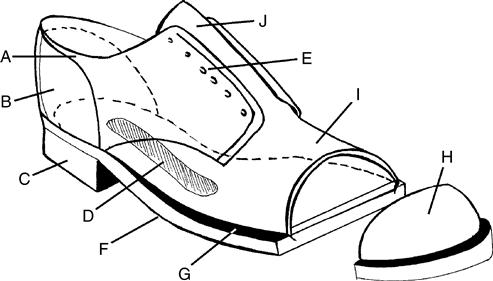
A suitable pair of shoes minimizes stress on all portions of the feet, provides support, and acts as a shock absorber of ground reaction forces.2 The basic parts of a shoe are the sole, upper, heel, and last. Each of these parts is further divided into component parts or areas that are required for proper shoe design (Figure 7-1). Each component is crucial to the prescription of appropriate shoes for the person’s individual needs.
Sole
The sole protects the plantar surface of the foot. The traditional sole consists of two pieces of leather sewn together with a layer of compressible cork between. An additional layer, the insole, is situated next to the foot in most shoes. A heavy thick sole protects the foot against walking surface irregularities. The rigidity or stiffness of the sole is also important. Although it needs to be durable, the sole must not be so rigid as to interfere with the toe rocker of the metatarsophalangeal (MTP) hyperextension during terminal stance and preswing phases of gait.
Various areas of the sole are identified by location. The welt is the inside piece of the external sole; the outsole is the portion that is most external. The area that lies between the heel and the ball of the shoe, the shank, is commonly fabricated to provide reinforcement and shape using materials such as spring steel, steel and leatherboard, or wood strips between the welt and the outsole. The purpose of the shank is to prevent collapse of the material between the heel and the ball of the foot and to provide extra support. In most athletic shoes, the sole is rubber to provide maximal traction. Rubber soles absorb shock, thereby minimizing heel impact forces.
Upper
The upper of the shoe—divided into the vamp, tongue, and rear quarters—covers the dorsum of the foot. The vamp extends from the insole forward. The tongue is an extension of the vamp in a blucher-style closure, but in the bal-type oxford, the tongue is separate (Figure 7-2). The blucher-style closure can be opened slightly more than the bal oxford closure to allow the foot into the shoe. The toe of the vamp is often covered with a separate piece of leather called the tip. The rearward line of the tip may be straight or winged. The vamp is joined to the quarters, which make up the sides and back of the upper. The two quarters are joined at a back seam. The design of the shoe dictates the shape and size of the quarters. For the oxford shoe, the outside quarter is cut lower than the inside to avoid contact with the malleoli. In the bal oxford, the back edges of the vamp cover the forward edges of the quarter. The forward edges of the quarters are on the top of the vamp in the blucher style of shoe.

For individuals wearing orthoses and those with foot deformity, the blucher closure is preferable to the bal-style closure because of its construction. The blucher closure has a separation between the distal margins of the lace stays, thus offering a wide inlet, making the shoes easier to don and doff and having a readily adjustable circumference. High shoes, which encase the malleoli, provide additional mediolateral stability.
Heel
The heel is located beneath the outer sole under the anatomical heel. The heel base is usually rigid rubber, plastic, or wood with a resilient plantar surface. As heel height increases, the ankle range of motion necessary to lower the forefoot to the floor increases. Weight-bearing pressures (vertical forces) on the forefoot and hallux also increase in midstance to late stance.3 The individual with limited ankle motion may benefit from a compressible heel base to absorb shock and achieve plantar flexion during the early stance phase. A broad, low heel maximizes stability and minimizes stress on the metatarsal heads. Most lower extremity orthoses and prosthetic feet are designed for a specific heel height; efficacy of the orthosis or quality of the prosthetic gait can be significantly compromised if used with shoes that have higher or lower heels.
Reinforcements
Strategic shoe reinforcements contribute to foot protection. Toe boxing at the distal vamp shields the toes and prevents the anterior portion of the vamp from losing its shape. The toe box can also be increased in depth to protect and accommodate any toe deformities. The heel counter reinforces the quarters to help secure the shoe to the anatomical heel. The medial counter helps support the medial arch of the shoe, and the heel counter aids in controlling the rearfoot. The convex shank piece stiffens the sole between the distal border of the shoe heel and the MTP joints and aids in supporting the longitudinal arch.
Lasts
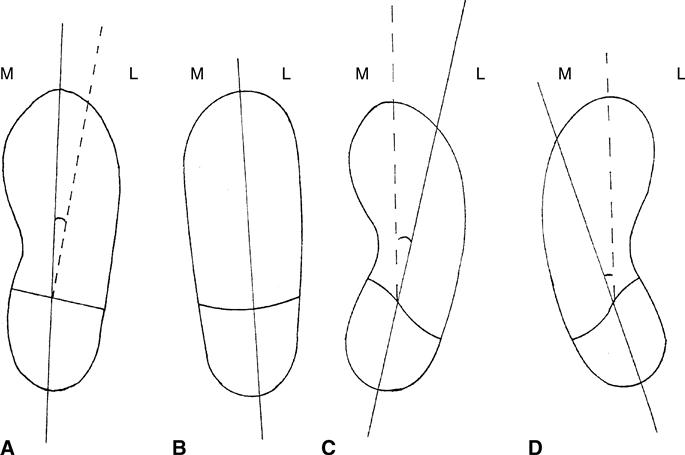
Shoes are constructed over a model of the foot, called a last, which is styled from wood, plaster, or plastic. Manufacturers are now converting to computer-aided last designs. Regardless of the origin of the last, it determines the fit, walking ease, and appearance of the shoe. Commercial shoes are made over many different lasts in thousands of size combinations. Most shoes are made with a medial last, which means that the toe box is directed inward from the heel (Figure 7-3). Shoes can also be made from conventional lasts, straight lasts, inflared or medial lasts, or outflared or lateral lasts.
Fashion versus function
A revolution to create comfortable and “healthy” shoes has occurred within the shoe industry in response to an epidemic of footwear-related health problems, the result of long-term wearing of improperly fitting shoes, which accounts for more than $3 billion annually in surgery-related costs.4,5 Even the most savvy, health-conscious women sometimes buy shoes for looks, not fit. A survey of 356 women concluded that almost 90% of women wore shoes that were one to two sizes too small.6 This trend contributes significantly to the development of bunions, hammertoes, claw toes, mallet deformities, corns and calluses, and other disabling foot problems in midlife and later life.7
Enhancing Function
Foot stability is critical to minimizing ankle injury, excessive pronation, and slipping of the heel during the gait cycle. A well-designed shoe provides a broad heel base, ankle collar, and close-fitting heel counter. A keystone of a good shoe is its ability to absorb shock. The construction of and materials used for the insole, midsole, and outer sole determine the amount of shock absorption that the shoe will provide.
A good shoe must be flexible and provide stability with each step. Flexible construction is especially important in the sole to enhance the toe rocker in late stance phase. The sole should also provide adequate traction as it contacts the ground, especially in early stance as body weight is transferred onto the foot. A coefficient of friction that is sufficient to minimize slips and near slips is vital. Heel height can create stress on the forefoot during gait. Heels of more than 11/2 inches exponentially increase weight-bearing forces on the metatarsal heads.7
The ability of a shoe to handle moisture is also an important consideration. For optimal foot health and comfort, perspiration must be wicked away and, at the same time, external moisture must be kept out.
The upper should be soft and pliable. Modern tanning techniques can create strong but supple uppers that surround the feet supportively and protectively without rubbing and chafing, while allowing the foot to breathe.
Orthotic-Related Function
A molded insole contributes to foot stability, shock absorption, and a transfer of shear forces away from problem areas. Orthoses can enhance the function of the shoes. Chapter 8 presents the principles and practices of orthotic prescription in commonly occurring conditions of the foot.
Proper fitting of a shoe: “if the shoe fits”
The two primary determinants of proper shoe fit are shoe shape and shoe size. Shoe shape refers to the shape of the sole and the upper. Proper fit is achieved when shoe shape is matched to foot shape. Shoe size is determined by arch length, not by overall foot length.8 The proper shoe size is the one that accommodates the first metatarsal joint in the widest part of the shoe. Properly fitting shoes are important in avoiding foot discomfort and deformity and are absolutely essential in individuals with arthritis, diabetes, and other foot disorders.
Great variability is found in human foot size and shape. Mass-produced shoes, however, are formed over fairly standard lasts that give a shoe its special size and shape. In the well-fit shoe, the shape determined by the last approximates the human foot. The design and construction of the shoe should allow for a roomy toe box; it should be wide enough for normal toe alignment and be 1/2 inch longer than the longest toe. Proper fit of the forefoot in the shoe can be a critical factor in reducing the incidence of bunions, hammertoes, and other forefoot deformities. In general, the shoe should be wide enough to accommodate the widest part of the forefoot. A tracing of the foot (standing) should fit within an outline of the shoe bottom.
Proper fit presupposes proper design, shape, and construction and is fundamentally wedded to availability in widths as well as lengths. It is important that the clinician cultivate a consumer mindset that realizes the medical importance of modifying the old cliché “if the shoe fits, wear it” to “if the shoe fits, wear it, and if it doesn’t, order it in the correct size.”
Determining Measurements
The average shoe salesperson does not offer to measure the foot, instead relying on the consumer to know his or her foot size. However, because foot size changes over time, periodic measurement of both feet for length and width is important. Many shoe styles that are available in retail shoe stores do not appropriately match the shape of an individual’s foot. As a result, comfort and protection are compromised in the name of “style.” This is especially problematic in the presence of foot deformity. Hallux valgus is a foot deformity that is aggravated by wearing shoes too narrow across the metatarsal heads and triangularly shaped in the toe box. Shoes should be wide enough to allow the material of the upper that surrounds the widest region of the forefoot (i.e., the metatarsal heads) to be compressed at least 1/16 inch before bony contact is made. Likewise, there should be at least a 1/2 inch between the tip of the longest toe and the front of the toe box in weight bearing (generally the width of the thumb).
In the United States, 12 standard shoe widths are manufactured. They range from the very narrow AAAAA to the very wide EEEE—that is, AAAAA, AAAA, AAA, AA, A, B, C, D, E, EE, EEE, EEEE. Because most retail stores stock shoes of midrange widths (A-E), patients with narrow or wide feet often have difficulty finding shoes of the optimal width.
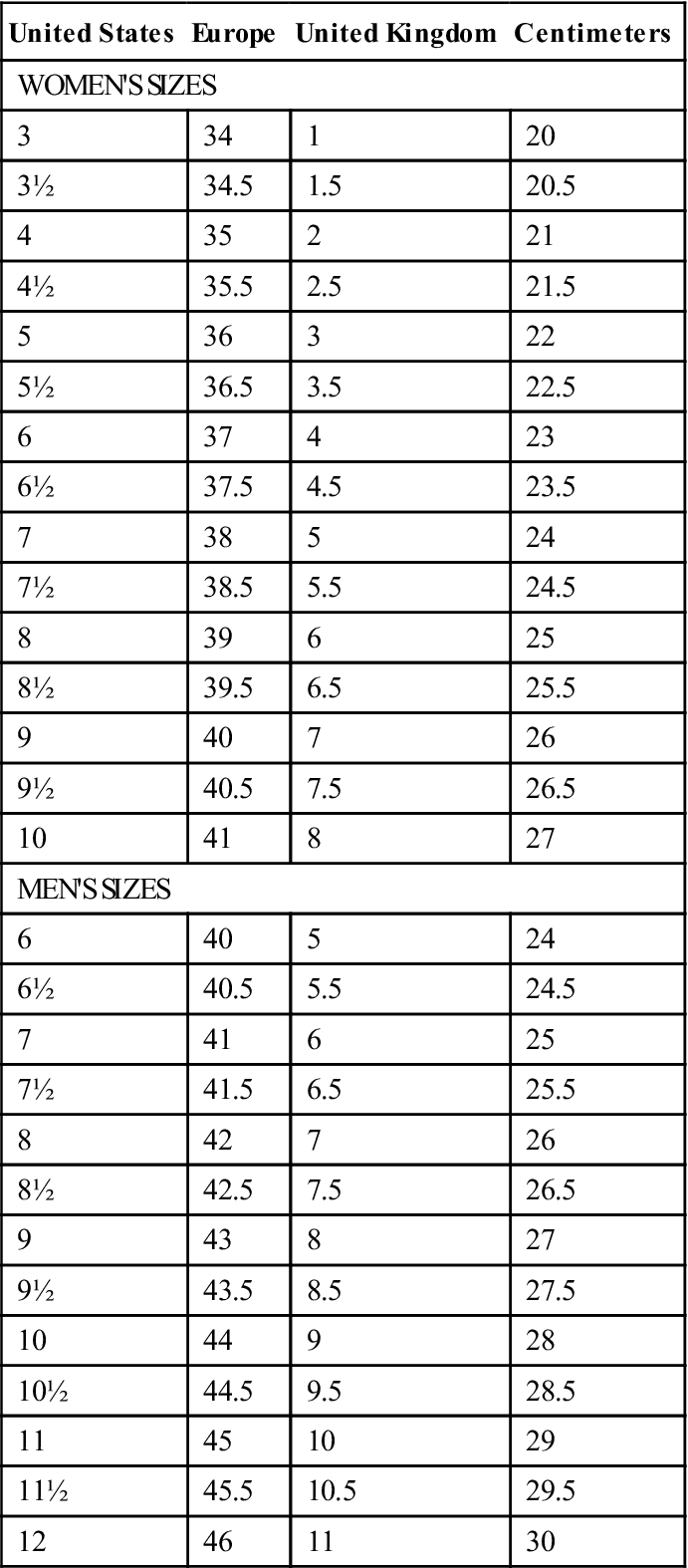
Standard shoe sizes are available in half-size increments, from an infant’s size 0 to a man’s size 16 in U.S. sizes. The difference in length between half sizes is 1/16 inch. Standard shoe-sizing classifications are made by groups and lasts: infants’ sizes 0 to 2; boys’ sizes 21/2 to 6; girls’ sizes 21/2 to 9; women’s sizes 3 to 10; and men’s sizes 6 to 12. Sizes larger than women’s size 10 and men’s size 12 must often be specially ordered. A U.S. women’s shoe size is usually three half sizes smaller than the corresponding men’s size (e.g., women’s size 9 is the same as a men’s size 71/2).
European and U.K. manufacturers use a different numbering system. The comparison of European and U.K. women’s to men’s sizes is based on centimeters (e.g., women’s size 38 EUR/5 UK is the same as men’s size 40 EUR/5 UK). Table 7-1 compares the standard sizes for U.S., European, and U.K. shoe manufacturers and lists the measures for each size.
Table 7-1
Comparison of Standardized Shoe Sizes
| United States | Europe | United Kingdom | Centimeters |
| WOMEN’S SIZES | |||
| 3 | 34 | 1 | 20 |
| 3½ | 34.5 | 1.5 | 20.5 |
| 4 | 35 | 2 | 21 |
| 4½ | 35.5 | 2.5 | 21.5 |
| 5 | 36 | 3 | 22 |
| 5½ | 36.5 | 3.5 | 22.5 |
| 6 | 37 | 4 | 23 |
| 6½ | 37.5 | 4.5 | 23.5 |
| 7 | 38 | 5 | 24 |
| 7½ | 38.5 | 5.5 | 24.5 |
| 8 | 39 | 6 | 25 |
| 8½ | 39.5 | 6.5 | 25.5 |
| 9 | 40 | 7 | 26 |
| 9½ | 40.5 | 7.5 | 26.5 |
| 10 | 41 | 8 | 27 |
| MEN’S SIZES | |||
| 6 | 40 | 5 | 24 |
| 6½ | 40.5 | 5.5 | 24.5 |
| 7 | 41 | 6 | 25 |
| 7½ | 41.5 | 6.5 | 25.5 |
| 8 | 42 | 7 | 26 |
| 8½ | 42.5 | 7.5 | 26.5 |
| 9 | 43 | 8 | 27 |
| 9½ | 43.5 | 8.5 | 27.5 |
| 10 | 44 | 9 | 28 |
| 10½ | 44.5 | 9.5 | 28.5 |
| 11 | 45 | 10 | 29 |
| 11½ | 45.5 | 10.5 | 29.5 |
| 12 | 46 | 11 | 30 |
Foot Contour
Foot contour changes throughout the life cycle. Aging, pregnancy, obesity, and everyday stresses on the foot cause it to widen. Deformities such as bunions increase the width and shape of the foot, and splaying of the metatarsal heads creates a collapse of the transverse arch, further increasing the width of the forefoot.9 Forefoot height may increase in the presence of toe deformities. Deformities such as pes planus (foot flattening) or pes cavus (high arches) change the contour of the midfoot. The shape of the foot must be considered and accommodated when an individual is measured for shoes. Often a “combined last” (where the last in the toe box is different from the rearfoot counter) is required to accommodate the contour of the foot. The relationship of the forefoot to the rearfoot is an important consideration in determining if the shoe shape, provided by the last, corresponds to the shape of the foot. Shoes with medial, straight, or lateral lasts can be ordered to best meet patient needs.
Obesity and Edema
The additional mechanical stress of carrying excess weight takes its toll on the feet, often resulting in problems such as plantar fasciitis, arthritis and bursitis, heel pain, neuroma, and gait changes.10 Frey and associates10 found that a weight gain of as little as 9 lb over a 5-year period increased foot size by one full size. Obesity has been shown to increase the length and the width of the foot. The Frey study also revealed that although women tended to adjust for length increases by purchasing a longer shoe, they rarely increased shoe width. The net result over the 5-year study period included increased incidence of calluses, corns, bunions, hammertoes, ingrown toenails, and neuromas.
Obesity also has an impact on gait patterns. Obese persons demonstrate increased step width, increased ankle dorsiflexion with reduced plantar flexion, increased Q angles at the knee, increased hip abduction angles, increased abducted foot angles, greater out-toeing, a tendency for flat-footed weight acceptance early in the gait cycle, increased touchdown angles, more eversion at the subtalar joint, and a faster maximum eversion velocity. These gait changes may be an attempt to increase stability during gait. The net effect, however, is an increased incidence of overuse injuries as a result of everyday activities.10
Proper shoe fitting is essential for preventing secondary foot problems that stem from ill-fitting shoes. Overweight individuals should be encouraged to have their feet measured regularly, particularly if they have had a significant weight gain. It is often helpful to shop for shoes at the end of the day, when feet are largest, and the shoe fitting should be done with the person standing to ensure that 1/2 inch is between the end of the longest toe and the edge of the toe box. The shoes should be comfortable the moment they are worn.
Fluctuation in foot size in individuals with edema (e.g., those with kidney dysfunction or congestive heart failure or any patient who is taking diuretic medication) creates a challenge when fitting shoes. The contour of the foot is constantly changing. For someone with severe edema, a Thermold (P. W. Minor Shoes, Batavia, N.Y.) Velcro closure shoe/sandal (Figure 7-4) is recommended to accommodate and support the foot and prevent the undue pressures imposed by a shoe that becomes too small during the course of the day.

Consequences of the ill-fitting shoe
The national obsession with beauty has created some not-so-beautiful feet problems, such as bunions, hammertoes, and neuromas. These are particular problems for women, who often select poorly fitting shoes in an attempt to have the foot appear to be smaller, daintier, and narrower than it actually is. In Frey and associates’ study,6 90% of women surveyed wore shoes that were too small by one or two width and length sizes, and 80% of these women had foot problems. Snow and associates11 report that 90% of 795,000 surgeries for bunions, hammertoes/claw toes/mallet toes, neuromas, and Taylor bunions could be directly attributed to wearing ill-fitting shoes. Foot problems including bunions, lesser toe deformities, and neuromas are the primary consequences of wearing ill-fitting shoes. Clearly, many of these problems would be prevented by habitual use of properly fitting shoes.
Special considerations
Feet come in many shapes, sizes, and conditions of health. The biomechanical and functional characteristics of feet change over an individual’s lifetime and must also be reflected in shoe choice. An infant’s foot must adapt to weight bearing, especially as walking becomes functional. The foot of a child continues to adapt as normal growth changes alignment of pelvis, femur, and tibia. The influence of hormones during pregnancy also affects the structure and function of the foot. Finally, the combined influence of the aging process, obesity, and diseases that are common in later life can create special footwear needs for older adults.
Pediatric Foot
Many pediatric and lower extremity foot disorders are minimally symptomatic and do not require treatment, whereas others require more aggressive management. An understanding of the natural history of many of these disorders is important in establishing the appropriate footwear for toddlers and children as they begin to walk and run.12–14
In-toeing is a problem caused by positional factors in utero and during sleep, muscle imbalances due to paralytic disorders, and decreased range of motion in the lower kinetic chain. It may also be due to metatarsus adductus, internal tibia torsion, or internal femoral torsion.
Metatarsus adductus is characterized by a bean-shaped foot that results from adduction of the forefoot. In most children (approximately 85%), this disorder resolves itself spontaneously.15 If it does not improve over the first 6 to 12 weeks of life, the treatment of choice is an outflared shoe. The bones of the foot are soft and can be corrected with positioning in the outflared shoe (reverse last) or Bebax shoe (Camp Healthcare, Jackson, Mich.).
Internal tibial torsion is a twist between the knee and the ankle. Generally, this torsion disappears by 5 years of age. Torsion can be exacerbated by abnormal sitting and sleep postures with the foot turned inward. (Some of the best athletes are in-toers.) The Dennis Browne bar or the counterrotation splint is used in combination with a reverse last shoe to remodel the bones during growth. Persistent severe toeing created by internal tibial torsion requires a derotational osteotomy of the tibia/fibula in the supramalleolar region.
Internal femoral torsion can also be the cause of in-toeing with a twist between the knee and hip. Neither splints nor shoes are effective in treatment of torsion. Habitual sitting in the “W” position (e.g., when a child is watching television or playing games on the floor) can aggravate the problem. Children with internal femoral torsion should be encouraged to sit “X” legged as an alternative.
Out-toeing occurs in children who sleep in the frog position and have soft tissue contractures around the hip. This is usually a hip or a long bone torsion problem and is not affected by footwear.
Toe walking can be the result of an in utero shortening or a congenital shortening of the Achilles tendon but can also be an early sign of cerebral palsy, muscular dystrophy, or Charcot-Marie-Tooth disease.15 Until 4 years of age, the ability to stretch the tendon is well preserved, and conservative treatment includes stretching, casting, ankle-foot orthoses, and/or a night splint. Z-plasty lengthening is performed if conservative interventions fail. Shoe prescription objectives follow the same principles as those in the older adult with Achilles tendinitis (see Achilles Tendinitis, Bursitis, and Haglund’s Deformity).
Flexible flatfoot appears to reflect generalized hereditary ligamentous laxity.16 Treatment for flatfootedness in children has changed over time. Currently, the shoe used to treat flatfoot is designed to correct heel valgus, support the arch, and pronate the forefoot in relation to the rearfoot. Forefoot pronation is achieved by using a lateral shoe wedge combined with a medial heel wedge. A scaphoid pad supports the arch, and a strong medial counter prevents medial rollover. A Thomas heel is often used to provide additional support for the arch.
Calcaneovalgus is a congenital positional deformity. The heel is in severe valgus, and the foot is dorsiflexed so much that it rests against the anterolateral aspect of the tibia. Calcaneovalgus is usually secondary to intrauterine position. Most cases correct spontaneously. Treatment of the severe cases includes stretching and serial casting. A few severe cases, if left untreated, persist into adolescence as pes planus.
An accessory navicular bone is a small ossicle at the medial tuberosity of the navicular. Individuals with an accessory navicular bone often complain of pressure and discomfort when wearing shoes. Often, placement of a prefabricated arch support in the shoe lifts the arch just enough to minimize rubbing on the shoe.
Hallux valgus (bunions) is most often the consequence of rearfoot valgus, leading to varus of the first metatarsal. The conservative approaches to treating this condition in children are orthoses and comfortable shoes, with a good heel counter to maintain the heel in subtalar neutral.
Curly toes involve the congenital shortening of the flexor tendons. Treated conservatively, flexors are stretched, and a rocker-like insole is used in the shoe to support the toes in extension. Shoes must have extra depth with plenty of room in the toe box.
Shoe prescription for these biomechanical problems of the foot and lower extremity in childhood is as valuable as a conservative corrective intervention. Overall, if a child’s foot is developing normally and does not exhibit any signs of an abnormality, a soft-soled shoe is appropriate.17,18 If some degree of abnormality exists, a more supportive, rigid shoe is indicated for toddlers. In general, the stiffer the heel counter, the more effective the intervention.
The most common prescription shoe for young children is a straight last shoe. This type of shoe is roomy enough to accommodate pads or wedges. In addition, a straight last shoe does not generate any abnormal forces against the child’s foot.
Foot During Pregnancy
During pregnancy, women may experience problems in lower extremities, including edema, leg cramps, restless legs syndrome, joint laxity, and low back pain. As a result, foot pain is a common problem in pregnant women.19 An important consideration is the provision of shoes with maximum shock absorption. Gel-cushioned running shoes are recommended, especially if women continue to jog or walk for exercise. Expectant mothers are also advised to exercise on soft surfaces to prevent problems caused by repetitive pounding on unforgiving surfaces.
High-heeled shoes exaggerate the lordotic curve and are inadvisable during pregnancy. As weight distribution shifts with advancing pregnancy, especially if edema occurs, many women choose to wear shoes with laces or a Velcro closure. Athletic and walking shoes provide good support, excellent cushioning, and a solid heel counter. If a heel is desired for special occasions, a 1-inch or lower heeled shoe should be recommended. Even low but tiny tapered heels cause women to wobble as they walk.
Many women find that their feet have “grown” during pregnancy; after having returned to prepregnancy weight and clothing, their shoes no longer fit. Measurements often reflect an increase in shoe length of a half to a full size. The stress of extra body weight coupled with ligamentous laxity can reduce arch height, adding length to feet. This process is a normal age-related change in foot structure, associated with wear and tear of the body over time, which is hastened during pregnancy. The hormonally induced tissue laxity of pregnancy leads to a broader forefoot as the metatarsal heads separate and the distal transverse arch flattens and to a longer foot as the longitudinal arch is less efficiently supported by soft tissue structures. For this reason, pregnant women are advised to wear a larger shoe size, with a square or deeper toe box, or both, especially if edema is also a problem.
Garbalosa and McClure20 found that almost 80% of the general population has a forefoot varum deformity. This foot deformity displaces the center of gravity forward, which can increase stress on the back during pregnancy. Forefoot varum deformity produces instability whenever the center of gravity is moved anteriorly over the forefoot in weight bearing, forcing the foot into exaggerated pronation.21 The net effect of the hormonal changes, pregnancy-induced forward displacement of the center of gravity, and the presence of forefoot varum is increased strain on the axial skeleton and reduced efficiency of gait. An orthosis to support the metatarsal heads and medial longitudinal arch, placed in shoes with good shock absorption ability, can help decrease foot discomfort and prevent injury to the low back during pregnancy.
Foot in Later Life
Foot problems are one of the most common complaints of older adults. The foot is also the most frequently neglected area of evaluation by most health care practitioners. In a study of patients who resided in a long-term care facility, 40% did not own properly fitting shoes. A subsequent survey indicated that the majority of community elders preferred to wear slippers and did not own adequate footwear.22
Gait disorders are a major cause of morbidity and mortality in older adults, significantly contributing to the risk of disabling injury.23 Gait changes, poor health, and impaired vision are the major predictors for falls.24 Many older persons attribute their problems with walking to pain or a sense of unsteadiness, stiffness, dizziness, numbness, weakness, or impaired proprioception.24
Physical therapists work with patients to maximize their functional abilities and mobility. Treating foot pain and dysfunction can be a fundamental contributor to becoming functional in ambulation. As Helfand so eloquently stated, “Ambulation is many times the key or the catalyst between an individual retaining dignity and remaining in a normal living environment or being institutionalized.”25
Gait and foot problems in older adults are associated with diseases that are common in later life and with the aging process itself. Examples of conditions that can compromise gait and foot function include the residuals of congenital deformities, ventricular enlargement, spinal cord diseases, joint deformities, muscle contractures, peripheral nerve injuries, peripheral vascular disease, cerebrovascular accidents, trauma, ulcers, arthritis, diabetes, inactivity, and degenerative and chronic diseases.23 The anatomical and biomechanical considerations of podogeriatrics focus on the interrelationships of the rearfoot, midfoot, and forefoot, established by osseous, muscle, and connective tissue structures. Movement of one joint influences movement of other joints in the foot and ankle. Soft tissue structures establish an interdependency of the foot and ankle to the entire lower limb. As tissues age, they become stiffer, less compliant, weaker, and more vulnerable to breakdown.
Foot contour alters with aging; the foot gets wider, and bunions and splaying occur from collapse of the transverse arch.26 Forefoot height increases in the presence of toe deformities. Fat pads under the metatarsal joints atrophy and shift position distally, whereas the calcaneal fat pad atrophies and shifts laterally. These changes leave bony prominences that are vulnerable to breakdown.
In the diabetic patient, development of Charcot’s joint (neuropathic arthropathy) is a relatively painless, progressive, and degenerative destruction of the tarsometatarsal or MTP joints.27–30 With the sensory losses that are common in diabetes, these joints are subjected to extreme stresses without the benefits of normal protective mechanisms. Capsular and ligamentous stretching, joint laxity, distention, subluxation, dislocation, cartilage fibrillation, osteochondral fragmentation, and fracture occur.31,32 Hyperemia increases the blood supply, which promotes resorption of bone debris with resorption of normal bone as well. The foot often fuses in a deformed rocker bottom shape, vulnerable to pseudoarthrosis, instability, abnormal weight-bearing surfaces, ulcerations, and infections.33,34
The majority of foot problems in geriatric patients can be managed with proper shoe fitting and minimal shoe modifications. The most inexpensive footwear for this patient population is running or walking shoes. These are less expensive and fit within a fixed-income budget.35 They provide good foot support and can be purchased with Velcro straps for closure if hand function or foot edema is a problem. The Thermold shoe is also a blessing for all the pathological and structural deformities with which the older patient must deal.
Choosing appropriate footwear and socks
A vast and somewhat bewildering variety of “off-the-shelf” footwear is available to consumers. Many shoes are designed with certain types of activities in mind. Understanding the design and construction, as well as ensuring proper fit, enhances foot health and minimizes the risk of foot dysfunction, injury, and pain.
Athletic Shoe Gear
Many people jump into fitness activities “feet first” and develop blisters, calluses, and other foot injuries because of inappropriate footwear. A well-fit, activity-appropriate athletic shoe enhances enjoyment of the activity by protecting and supporting the foot and minimizing injury. Athletic shoes are designed for specific activities. A running shoe is designed with a high-force heel impact and forward foot movement in mind; the various shoe models have specific features that are designed for different surface conditions and distances in running. Basketball shoes do not provide as much cushioning as do running shoes but instead focus on foot support during quick lateral movement. Aerobic shoes are also designed for lateral movement but provide more cushioning for the impact anticipated on the ball of the foot. Shoe soles are also designed for the surface on which the activity is performed. Some shoes are manufactured as cross-training shoes so that they can go from the workout in the gym to jogging but are not designed for high-mileage runners.
Determining the foot type is important in prescribing the best shoe. For individuals with a flat, low-arched foot, a shoe that provides maximum stability to prevent the foot from rolling in with each step is required. High-arched feet demand a shoe that is more flexible. “Normal” feet do best in a shoe that combines the last to accommodate the heel and the forefoot and that has forefoot flexibility. The size and shape of the toe box must also be considered. Enough room should be available in the toe box to prevent blisters, ulcers, and chafing of the toes. Shoes made from materials that “breathe” so that perspiration can escape are desirable. Athletic shoes are best used only for their intended activity and should be replaced at regular intervals to maximize their effectiveness.
Most athletic footwear is available in medium widths, although a few manufacturers provide shoes in several widths. Children’s athletic footwear is available in narrow, medium, and wide widths. Women’s athletic footwear may be available in AA, B, and D widths. Men’s athletic footwear may be available in B, D, EE, and EEE widths. The key element in proper fit of athletic shoes is comfort from the moment the shoe is put on, with no break-in period needed. The shoe should also provide adequate support and shock absorption for the sport or activity that is being pursued.
Walking Shoes
A well-designed walking shoe provides stable rearfoot control, ample forefoot room, and a shock absorption heel and sole. This type of footwear may be specifically designed by an athletic footwear manufacturer or even by an orthopedic footwear manufacturer. Walking shoes are available in various widths and in several different lasts. Long medial counters, Thomas heels, and crepe soles can be used to modify this type of shoe gear to meet specific patient needs.
Dress Shoes
Despite the fashionable preference for shoes with narrow or pointed toes and slim high heels, the most foot-friendly dress shoe for women is a rounded-toe Mary Jane style with boxy heels. A good dress shoe approximates the shape of the individual’s foot and provides flexibility and sufficient shock absorption. Prerequisites of a good dress shoe include a roomy toe box, low stable heel, proper width in the ball of the foot area, flexible outsole with skid-proof bottoms, and arch support.36
Triangular toe boxes and high heels, no matter how dainty, are best avoided because they can and do cause deformity. For a high-heeled shoe to stay on the foot, it must fit closely around the toes, resulting in no room for anything but the foot. The foot is virtually unsupported at the distal end of the shank, and extreme high pressure is present under the metatarsal heads. Heels higher than 2 inches make any kind of orthosis ineffectual.37 Because the angle of the foot causes the heel of the orthosis to lift up, high heels can transform an orthosis into a catapult. Although orthoses can help relieve metatarsal and heel pain and provide arch support, they cannot offer any corrective features in a shoe that is designed so unnaturally for the human foot.11
Socks
The sock is often overlooked when shoes of any kind are prescribed. Socks can aid in shock absorption, shield the skin from abrasion by the shoe stitching and lining, and prevent skin irritation from shoe dyes and synthetic leather materials. Additionally, clean, freshly laundered socks are integral to a sanitary foot environment. Unbleached, white cotton socks are ideal because they lack dyes, are hypoallergenic, and absorb perspiration readily. Cotton socks also provide ample toe room, unlike socks that are made from stretchable fabric, which can crowd the toes.
The size and style of socks also influence foot health. Socks that are too short crowd the toes; those that are too long wrinkle within the shoe, creating potential shear pressure points. If knee-high socks are worn, the proximal band must not be unduly restrictive; similarly, the use of circumferential garters to hold socks can impede circulation to the foot. Any holes worn into the sock also potentially create shear pressures and should be discarded. Mended holes in socks, because of the difference in thickness and materials, can irritate delicate or insensate soft tissue. An open hole at the toes pinches and constricts the digits, with excessive friction at the edges of the hole.
The Thor-lo sock (Thor-lo Inc., Statesville, N.C.) is specially designed to support and cushion the insensitive foot or athletic/military foot that is exposed to repetitive frictional forces. Use of these specially designed socks not only reduces the frictional shearing forces but also significantly decreases vertical ground reaction pressure forces, preventing blistering and ulceration.38–43 Extra high-density padding functions as a natural fat pad, reducing the deteriorating effects of shearing forces and the pressure and friction in the toe area. The Thor-lo concept of stockings is beneficial for patients with insensitive feet. It has also been used for individuals involved in aerobic exercise, baseball, basketball, cycling, golf, hiking, trekking and climbing, skiing, tennis, walking, and running.
Prescription footwear, custom-molded shoes, accommodative molded orthoses, and shoe modifications
Alteration of foot function and alignment can be accomplished with one or more of the following strategies: foot orthoses of the appropriate materials, prescription shoes, and modifications of shoes themselves.44–46 These strategies are used to relieve pain and improve balance and function during standing and locomotion. These alternatives are indicated when a transfer of forces from sensitive to pressure-tolerant areas is needed to reduce friction, shock, and shear forces; to modify weight transfer patterns; to correct flexible foot deformities; to accommodate for fixed foot deformities; and to limit motion in painful, inflamed, or unstable joints.
When special protective or prescription footwear is being considered, the functional objectives must be clearly stated so that the appropriate specific prescription can be developed. Careful examination of the foot helps the clinician identify pathology or mechanical factors, or both, that must be addressed and choose the appropriate materials and footwear styles to meet the patient’s specific needs.
Moldable Leathers
Thermold is an example of prescription footwear that can be used to protect feet that are vulnerable due to vascular insufficiency, neuropathy, or deformity (Figure 7-5). It is a cross-linked, closed-cell polyethylene foam laminated to the leather upper of the footwear that can be heat molded directly to the foot. This makes modification for foot deformity easily managed and far less expensive than custom molding. Thermold shoes are also available in extra-depth styles, with a removable 1/4-inch insole. Extra-depth shoes enable adequate room for custom-made insoles or orthoses to become an intricate adjunct to the footwear. In some instances, the Thermold can be used as an alternative to the custom-molded footwear.
< div class='tao-gold-member'>

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


