FIGURE 26-1. A: Radiograph of failed total hip arthroplasty with femoral component loosening. B: Radiograph after reconstruction with Wagner nonmodular body fluted tapered stem.

FIGURE 26-2. Wagner revision stem: the progenitor of modern fluted tapered grit-blasted titanium revision implants.
HOW FLUTED MODULAR TAPERED STEMS WORK
Fluted tapered modular stems work on the principle that the diaphysis of the femur can be milled to become a supportive tapered cone of bone. Engagement of the conical stem into the conically reamed femur provides axial stability of the implant. Sharp flutes provide rotational stability of the stem (Fig. 26-2). These stems are made of titanium or titanium alloys that have a grit-blasted surface. This surface texture promotes bone ongrowth and has been demonstrated to provide long-term biologic implant fixation.
Modern fluted tapered stems have a modular body, which has markedly enhanced the success of these implants. The femur is reamed distally to a supportive cone, and the distal conical fluted section of the stem is impacted into the femur until it is axially and rotationally completely stable. Subsequently, a proximal modular body, which provides optimal leg length and femoral offset, is then attached to the upper stem. The modularity of these systems allows the surgeon to simultaneously optimize complete seating of the implant into the tapered cone of bone and also restore hip biomechanics and hip stability.
The modular junction of these stems is in the high stress subtrochanteric area of the femur2 (Fig. 26-3), and consequently, the junction is subject to metal fatigue failure. Fracture of a number of different devices at their junctions has been reported, and manufacturers have worked to optimize the strength of stems in this area to minimize the risk of this failure mode.

FIGURE 26-3. Radiograph of fractured taper junction of modular body stem. The modular junction is in the high stress subtrochanteric area of the femur.
Because fluted tapered stems are titanium, they are less stiff (for a specific stem diameter) than a fully porous-coated cobalt-chromium stem. Reduced modulus of elasticity has the theoretical advantage of reducing stress shielding of the proximal bone. Several reports on fluted tapered stems make note of bone reconstitution after reconstruction with these implants, although the local bone mass changes have not been rigorously quantitated.3–5 Some of the observed bone reconstitution may be due to bone recovery after removal of a failed implant, and some may be due to a fracture healing effect associated with extended osteotomies. Nevertheless, the bone remodeling pattern around these stems appears to be different than that observed around extensively porous-coated stems (Fig. 26-4). Possibly the combination of a lower modulus of elasticity in association with a grit-blasted surface (which may promote less intense bone in-growth/ongrowth at the most distal aspect of the stem compared to extensively coated uncemented stems) explains some of the favorable bone remodeling around these implants.

FIGURE 26-4. A: Radiograph of failed total hip arthroplasty. B: Radiograph 4 years after revision demonstrating excellent bone remodeling. Cancellous intramedullary grafting was also performed at revision.
Indications for use of these stems vary according to the surgeon’s philosophy. Some surgeons use these stems for most of their revisions, while others selectively use them in circumstances not ideal for other revision implants. Fluted tapered modular stems are particularly valuable when there is sufficient damage to the bone that good axial support for a long parallel-sided extensively porous-coated uncemented implant is not present (Figs. 26-5–26-7). Fluted tapered stems also may be used in Paprosky type IV bone defects in which the diaphyseal section of bone is too short to provide reliable bone ingrowth into an extensively coated parallel-sided stem. However, there must be sufficient bone present for the surgeon to create a supportive cone of bone; otherwise, the implant will subside (Figs. 26-8–26-10). Fluted modular tapered stems are particularly valuable for treating periprosthetic femur fractures (see Chapter 32). Finally, some surgeons use fluted tapered stems when there is complete loss of proximal bone stock, much like a tumor prosthesis. It remains to be seen whether the modular tapers of these implants are sufficiently strong for use in this manner.
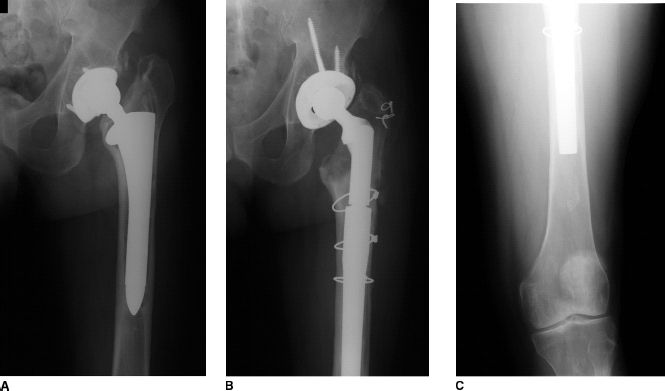
FIGURE 26-5. A: Preoperative radiograph of failed total hip arthroplasty. Note deficient proximal bone and large canal diameter. B,C: Postoperative radiograph after revision with fluted tapered stem. Note that the femur has been milled to tapered cone.
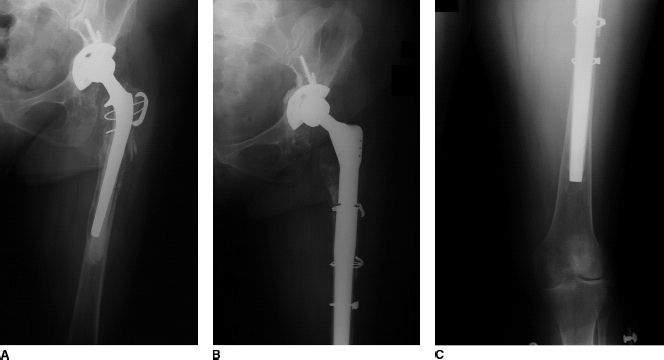
FIGURE 26-6. A: Preoperative radiograph of failed total hip arthroplasty. Note markedly deficient proximal bone. B,C: Postoperative radiographs after revision with fluted tapered stem. Note that the femur has been milled to tapered cone and a corrective proximal osteotomy performed.
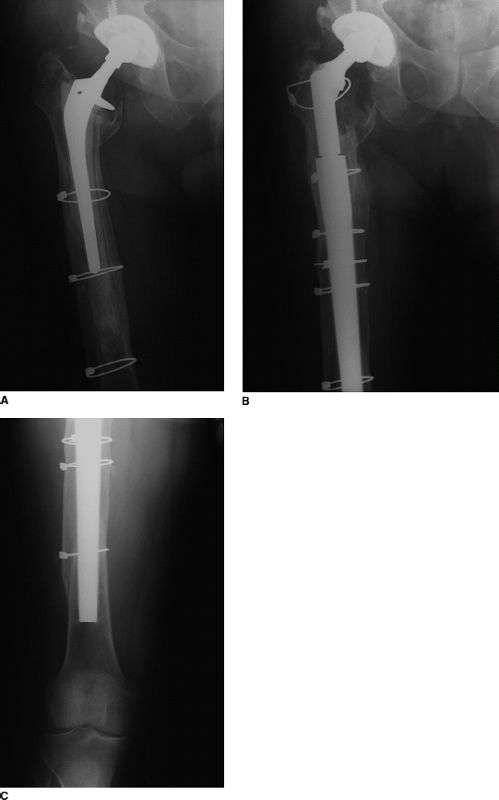
FIGURE 26-7. A: Preoperative radiograph of failed total hip arthroplasty. Note large canal diameter. B,C:
Related posts:
 Venous Thromboembolism Prevention
Venous Thromboembolism Prevention
 Postoperative Rehabilitation After Total Knee Replacement
Postoperative Rehabilitation After Total Knee Replacement
 Proximally Porous-Coated Modular Stems
Proximally Porous-Coated Modular Stems
 Critical Decisions in Revision Total Hip Arthroplasty
Critical Decisions in Revision Total Hip Arthroplasty
 The Use of Cages in Revision Arthroplasty of the Acetabulum
The Use of Cages in Revision Arthroplasty of the Acetabulum
 Postoperative Periprosthetic Femur Fracture Around Total Hip Arthroplasty
Postoperative Periprosthetic Femur Fracture Around Total Hip Arthroplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


