3
Flexibility and Stretching
1. Describe viscoelasticity and the properties associated with collagen.
2. Explain the stress-strain curve and factors that influence change.
3. Discuss Golgi tendon organs (GTOs) and muscle spindles.
4. Discuss how temperature affects connective tissue.
5. Define and discuss range of motion, flexibility, and stretching.
6. Outline various methods used to measure flexibility.
7. Identify and describe various stretching techniques.
8. Discuss precautions and essential components of stretching program development.
9. Discuss at least two proposed benefits of stretching.
10. Explain how stretching might negatively impact activity performance.
11. Describe the clinical applications for stretching soft-tissue contractures.
12. Describe and contrast the differences and similarities between scar tissue and adhesions.
Enhancing flexibility is an important component of a fitness program7 and is useful, not only for sport-specific activities, but also for activities of daily living (ADLs). The need for flexibility is particularly necessary if mobility has been impaired, resulting in compromised range of motion (ROM). ROM is the amount of movement available to a joint moving within its anatomic range. Muscular imbalances due to shortened muscles may lead to faulty postural alignment that may lead to injury and joint dysfunction. The ability to restore ROM is crucial when implementing or following a rehabilitation program; consequently, being able to incorporate stretching exercises to restore flexibility as well as normal ROM and function becomes a primary goal for the physical therapist assistant (PTA).
Many clinicians emphasize that having a more flexible body is more efficient, improves muscle balance, and more easily undergoes strength and endurance training. Overall purported benefits of flexibility due to stretching include injury prevention, quicker recovery from workouts, a reduction in post exercise soreness, and facilitation of relaxation.2,129 However, the effects of stretching on performance is somewhat more controversial. Some literature shows that it may potentially help improve performance,48 whereas other literature and research reveal potential detrimental effects on maximal performance activities after stretching.66,113,124,131 Research into flexibility and stretching is ongoing in an attempt to determine the effects of stretching on the body. Consequently, some of the long-held beliefs about stretching, especially regarding performance, are being challenged.
PROPERTIES OF CONNECTIVE TISSUE
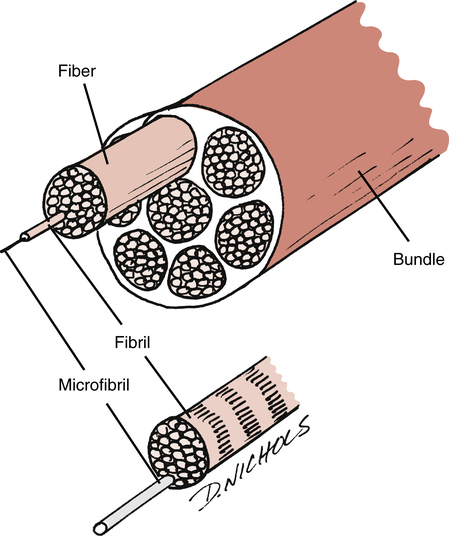
Just as amino acids are the building blocks of protein, tropocollagen is the building block of collagen (Fig. 3-1). Collagen fibers are made of short subunits (fibrils) and are found in varying amounts within the different connective tissues: bone, tendon, muscle, skin, hyaline cartilage, and joint capsule.20,41,119 Collagen is a protein building block of connective tissue and it provides the strength needed to withstand high levels of tension and force during movement and exercise. There are more than 20 types of collagen, but the majority of the collagen in the body consists of types I, II, and III.38 Of these, type I collagen is the most abundant in the body.
Type I collagen fibers are thick fibers gathered into bundles and display very little elongation when placed under tension (they have an ability to resist pulling). Type II collagen fibers, on the other hand, are thinner and possess slightly less tensile strength. These fibers are observed primarily in tissues such as articular cartilage and the nucleus pulposus. Type III collagen serves mainly in a structural support capacity and is found in expansible organs (e.g., arteries, liver, lungs).58 It is also common in fast growing or healing tissue and is often seen at the early stages (phase 1) of wound repair. It is later replaced by the tougher type I collagen.90
Elastin is a structural protein present in tendons in amounts of less than 1%.35,136 Tissues with greater amounts of elastin usually demonstrate greater degrees of flexibility. Elastin assists collagen in the recovery of tissues after stress.
Stress and Strain
Stress or load is given in units of force/area, where the units may be pounds per square inch or Newtons per square centimeter.96 Therefore stress is directly related to the magnitude of force and inversely related to the unit area, but is independent of the amount of a material.97 The complementary measure related to stress is strain or deformation. Strain is usually dimensionless, since the units of measure cancel each other out, but units are often provided (e.g., inches/inch) to give a perspective of scale applied to the loads.96
The relation of stress and strain is dependent on several factors. These include the material properties used, the magnitude of the stresses, and the rate of stress application. Subsequently, the graphical representation of stress and strain is different for each type of material discussed. This representation is known as the stress-strain or load-deformation curve.92 Figure 3-2 demonstrates the various regions within the stress-strain curve, with each region demonstrating a biomechanical property of a tissue.
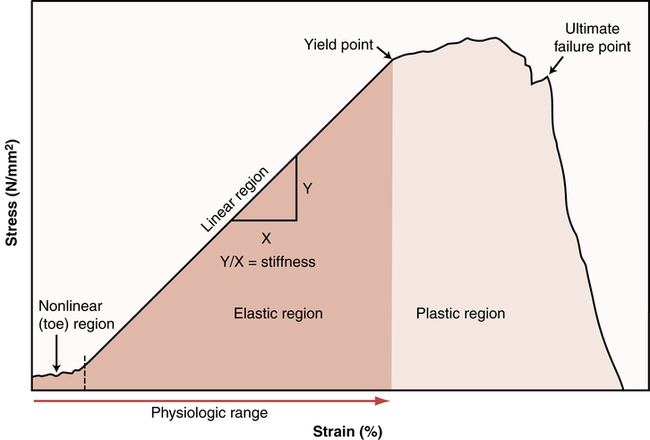
The toe region represents how a slightly pulled tissue (i.e., a ligament) produces only a small amount of tension within the tissue; it indicates that the collagen fibers within the tissue must first be pulled tight before a stretch can be induced. This minimal amount of tension simply results in the slack of the tissue being taken up with no stretch being encountered. The elastic region represents a linear change in strain, which occurs if the tissue continues to be pulled at higher stress levels. A good example of this linear relation is similar to the model of a stretched rubber band. The greater the load on the rubber band, the more the rubber band stretches. So, as the tension on the rubber band is removed, the band shortens, nearing its original length. Given this behavior, it is referred to as the elastic zone. The amount of stretch (strain) applied to the tissue in this zone is generally experienced during many body movements. Note that the slope (the angle of the curve) in this zone is indicative of the relative stiffness of the tissue. Stiffness is defined as the change in force per unit change in length.41 As such, the stiffer the tissue, the steeper the slope. So tissues such as ligaments will only change length at higher levels of stress compared with tissues of less stiffness, such as loose connective tissue.
The upper level of the elastic region marks a transition from the linear slope to one where the slope begins to flatten. This is called the plastic region and is a point where an increasing level of stress on the tissue results in proportionately increased changes in tissue length, probably due to microscopic failure of the tissue. This is termed the plastic zone because of the tissue damage resulting in permanent deformation (plastic deformation). Unlike the elastic region, the plastic energy is not recoverable in its entirety when the load is removed; additionally, there is a change in its resting length. Continued stretch in the plastic region would result in additional deformation of the tissue and would occur until it reached its initial point of failure. The toe region can include strains up to 3%; the elastic region, from 6% to 10%; and the plastic region, from 10% to 15%.41,112
Viscoelasticity
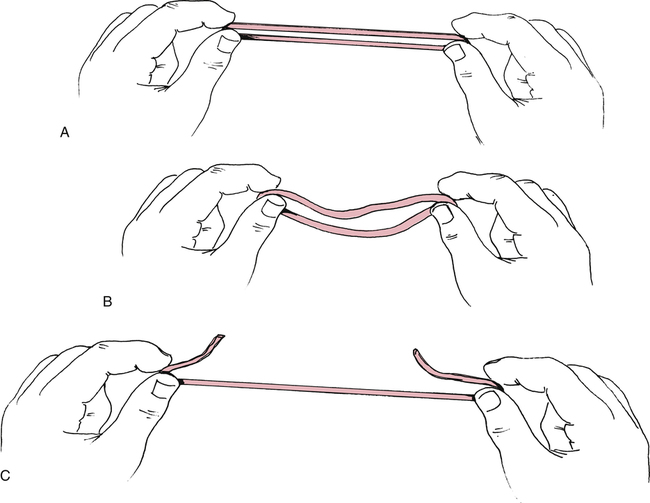
All connective tissue exhibits the property of viscoelasticity, which is simply a combination of the behavior of the properties of elasticity and viscosity.73,76 Elasticity refers to a material’s ability to return to its original state following strain or deformation (i.e., change in length or shape) after a removal of the stress or load. This mutable change is termed elastic deformation and is similar to the changes that occur in a rubber band under high rates of strain. The rubber band rapidly conforms to a new length and is able to return to its original resting length when the stress is removed. However, the rubber band breaks if the degree of stress exceeds the strain capabilities (Fig. 3-3). Viscosity refers to a material’s ability to resist a change in form or to dampen shearing forces. Tissues exhibiting viscosity have time-dependent and rate-dependent properties when forces are applied to them.
The rate at which tissues are stretched has a profound effect on the degree or percent of strain. As mentioned, tensile (distractive) or compressive forces will produce deformation on viscoelastic materials, but will allow return to their original state after removal of the force. Given normal conditions, however, viscoelastic materials do not immediately return to their original state. Viscoelastic materials, unlike pure elastic materials, have time-dependent properties. Slower rates of stress produce greater amounts of strain or elongation, whereas faster rates of stretch produce much smaller amounts of elongation.29,35,119 As such, they are sensitive to the applied force duration. Tissues gradually lengthen when they are subjected to constant or repeated stress of long duration.
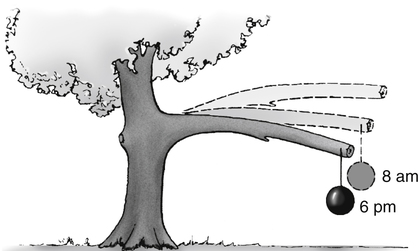
So a viscoelastic material subjected to either a constant compressive or tensile load will initially respond by rapidly deforming; it continues to deform over a finite length of time even if the load remains constant. This deformation of the tissue will continue until a state of equilibrium is reached when the load is balanced. This is called the creep phenomenon (Fig. 3-4),76 which simply means the gradual increase in tissue length that occurs when maintaining a constant stress (or force). For example, if one uses a constant force against the muscle with slow and passive stretching, the muscle will eventually elongate. However, the tissue does not return to its original length immediately when unloaded because of the collagen’s viscous property.73 Essentially, the longer the duration of the applied force, the greater the deformation or stretching of the tissue.
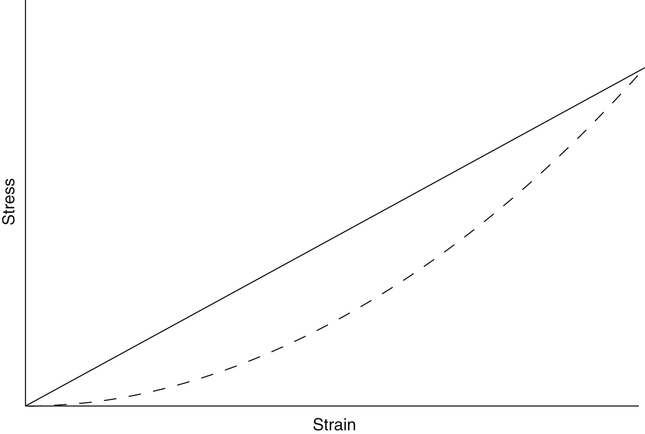
The loading and unloading of tissue is influenced by its viscoelastic properties. This loading and unloading is quantified by measuring the hysteresis area (Fig. 3-5). The loading (solid line) and unloading (dashed line) phases represent a measurement of the stress and strain that is applied to a tissue and then released. The hysteresis area lies between the two lines and represents the amount of energy dissipated in the loading and unloading process.41,73
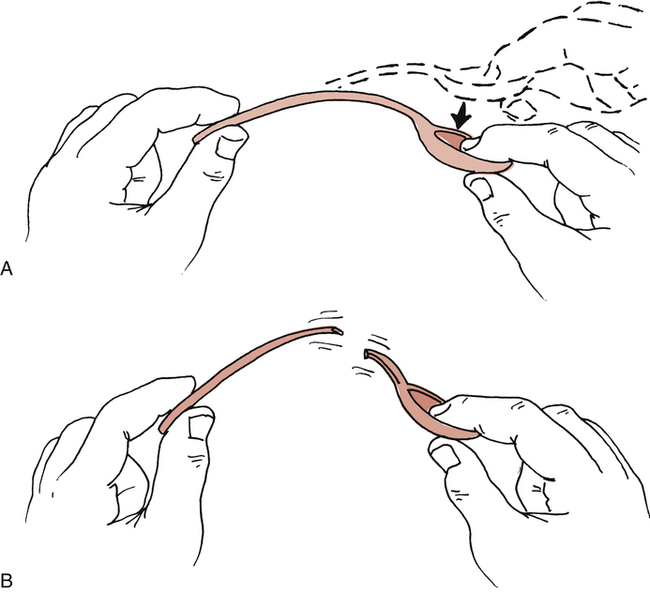
The ability of tissues to recover after stress is extremely important in relation to flexibility. Woo and colleagues136 have shown that increasing the levels of stress produces an increase in collagen within ligaments and tendons, whereas reducing the levels of stress causes weakening in connective tissues. Recovery is the ability of tissues to return to their previous resting state. However, it does not imply that permanent elongation or microscopic damage has not occurred. Plastic deformation is force dependent under slow rates of stress and is used to describe permanent change in a tissue. For example, when a low degree of stress is applied to a plastic spoon, the spoon slowly deforms to a new shape. The spoon breaks if the stress is applied too fast (Fig. 3-6). Lehman and colleagues74 and Warren and co-workers126 have demonstrated that recovery of the tissue’s resting length had occurred after microscopic failure had begun.
Along with stress and the rate of stress applied to tissues, temperature also affects connective tissue extensibility as well as the rate of creep. High temperatures in the range of 37° C (98.6° F) to 40° C (104° F) affect the viscoelastic properties of connective tissue and increase the rate of creep.29,73 The higher the temperature (approximately 45° C [113° F] is the therapeutic upper limit), the greater the degree of elongation with stress before tissue failure.108 Because connective tissue’s viscoelastic and plastic changes occur at higher temperatures, there is less microscopic damage under stress at these temperatures. Studies by Warren and colleagues127 have demonstrated that a temperature of 45° C is needed to reduce tissue damage during strains of 2.6% or less. So to stretch out a connective tissue structure, one should heat it and use a large load over a long period of time to produce creep.96 Low temperatures decrease the rate of creep.
Muscle or contractile tissue responds to stretch by elastic and plastic deformation properties in ways similar to connective tissue. Obviously the contractile properties of muscle allow for the greatest degree of freedom of movement around a joint. Although connective tissue is considered a passive resistant to joint motion, muscle tissue is considered an active restraint to joint motion by virtue of its elastic and contractile elements. Active exercise (muscular contractions) affects intramuscular temperature. Increases to approximately 39° C are observed in exercised muscle.6 Commonly used passive thermal agents that increase tissue temperature are moist heat and ultrasound. The judicious use of active exercise and passive thermal agents before and during stretching programs enhances the effectiveness of the prescribed program.
FLEXIBILITY
Kisner and Colby64 define flexibility as the ability of a muscle to relax and yield to a stretch force. Others have defined flexibility as the ability to move muscles and joints through a full ROM.12,102 In essence, flexibility refers to the degree of normal ROM available. Therefore, flexibility can refer to various measurable components of joint motion. Muscles, tendons, ligaments, skin, joint capsule, and bone geometry all influence the degree of movement in joints. For example, a muscle can stretch or elongate, creating a measurable effect on the joint or joints upon which it acts. If a muscle becomes damaged by trauma or disease or becomes shortened because of immobilization, its ability to stretch and allow freedom of joint motion is affected. Flexibility will diminish over time if tissues are not stretched or exercised using regular and proper stretching regimens.2 As such, the goal of any flexibility program would be to improve or maintain ROM at all joints.
Different classifications of flexibility currently exist, depending on how the tissue is stretched. For example, static flexibility occurs as a result of static stretching, whereas dynamic flexibility relates to moving through a ROM with normal or rapid velocity.2 However, evidence does not support the existence of flexibility as a single general characteristic of the body. Instead, it is specific to particular joints, joint actions, or movements and is highly variable among different individuals.53 An understanding of the properties and components of various connective tissues is fundamental in delivering various stretching and flexibility regimens.
Measuring Flexibility
It is important to assess overall flexibility by measuring ROM at specific joints, because no one composite test provides an index of an individual’s flexibility characteristics.53,54 Subsequently, some measurements of overall flexibility are somewhat difficult, since they involve a complexity of movements over several joints (e.g., sit and reach test).
Measuring joint ROM is accomplished by using standard goniometric instruments. The measuring device most commonly used to measure ROM is the universal goniometer (Fig. 3-7), which is a protractor with degree measurements. The goniometer arms are placed along the proximal and distal components of a joint with the axis centered over the joint, which are then moved in accordance with the body part being measured. The goniometer can be used to measure joint position and ROM at almost all joints of the body.95 Other types of goniometers used less frequently in the clinical setting are the inclinometer, the pendulum goniometer, and the fluid goniometer.

Consistency in measurement is crucial; therefore it is important to use the same type of goniometer for a specific patient each time that patient is measured. Because different goniometers may provide slightly different results, they should not be interchangeable in their use in the clinical setting. For example, when using an inclinometer as the measuring device, it should be used for all future measurements for that patient to ensure consistency.96 For documentation purposes, most authorities recommend using goniometry rather than visual estimates because of its increased accuracy and reliability of measurement.128,137
Joint stability differs from joint ROM in that the ligaments and surface geometry of joint articulations dictate static joint integrity (stability). A patient may demonstrate limited ROM in knee flexion and extension (by goniometry); however, anterior and posterior joint mobility may be excessive and unstable (Fig. 3-8). On the other hand, a patient may demonstrate normal joint ROM, yet when tested statically the joint may be very stable, tight, and unyielding to pressure.

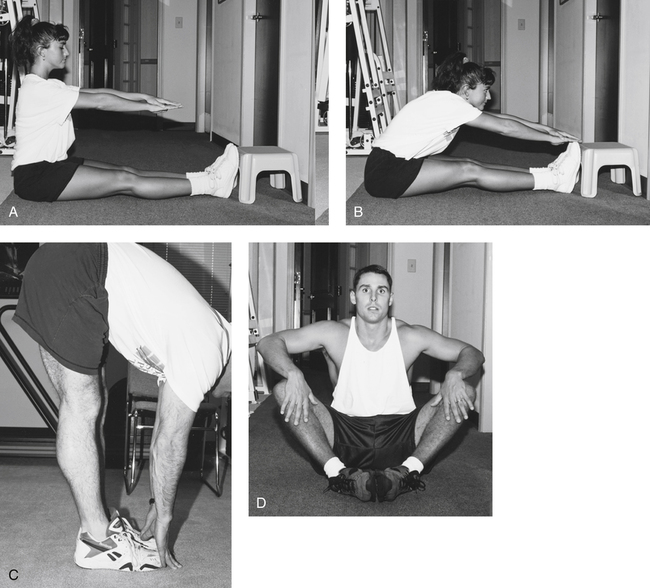
The sit and reach test (Fig. 3-9, A-B), standing toe touch for back and hamstring flexibility (Fig. 3-9, C), seated hip external rotation test (Fig. 3-9, D), and standing knee recurvatum test generally are less specific flexibility tests. These tests and others are used to provide very general assessment of multijoint flexibility. Such tests also can be used as stretching techniques to improve limitations in movement. However, objective clinical documentation of joint ROM is made by joint goniometry.
Factors Affecting Flexibility
In addition to muscles, tendons, and their surrounding fascia, other structures, such as bone, fat, connective tissue lesions, skin, and postural problems, may all lead to flexibility and joint ROM limitations.5 Other factors that may affect flexibility are age and gender.14,25
STRETCHING
Stretching involves elongating the muscles and tendons to the end of the available ROM. As such, applying a tensile force to a muscle results in a transient deformation, which elongates the musculotendinous unit, resulting in a stretch.2,40 Given that the mechanical behavior of connective tissue is primarily influenced by the amount of collagen available,73,119 the amount of stretching that takes place is dependent on the type of connective tissue present (i.e., skin, fascia, ligaments, tendons, joint capsules, and muscle fascia).
Although gradually increasing flexibility to increase ROM is the main goal, other adaptations occur from a regular stretching program. For example, research has shown that as a result of training, the stretch reflex may be reset to a different level.133,134 Several types of stretching exercises have been detailed in the literature and will be described in this section.
Stretching Principles
Stretching is effective primarily because of its mechanical and neurophysiologic effects.69,119 As mentioned, the muscle-tendon unit responds viscoelastically during stretching. However, some stretching exercises are based on the neural inhibition of the muscle undergoing stretch as well. In this case, a decreased reflex activity would result in reduced resistance to stretch, resulting in further gains of joint ROM. Most likely, both mechanisms are responsible.
It is important to note that stiffness relates to a tissue’s ability to resist stretch and indicates the amount of deformation proportional to the load applied.81 So, the stiffer the tissue, the less compliance it has and the less likely it is to stretch; conversely, less stiffness means greater compliance. It stands to reason then that flexibility training is designed to decrease the stiffness of the muscle-tendon unit.69,119 Furthermore, a rapidly applied stretch results in a greater resistance to that stretch.
Both mechanical and neurophysiologic components are inherent within muscular flexibility.43,50,105,118,119 However, some researchers believe that the ability of stretching to produce greater flexibility is primarily a result of the viscoelastic nature of muscle and connective tissue.84,119 As such, the most resistance to stretching probably is due to the connective tissue framework and sheathing from within and around the muscle and not the muscle itself (since the muscle itself can be stretched to 150% of its resting length); this includes the epimysium, perimysium, and endomysium and may even include the sarcolemma.107,109,116,117
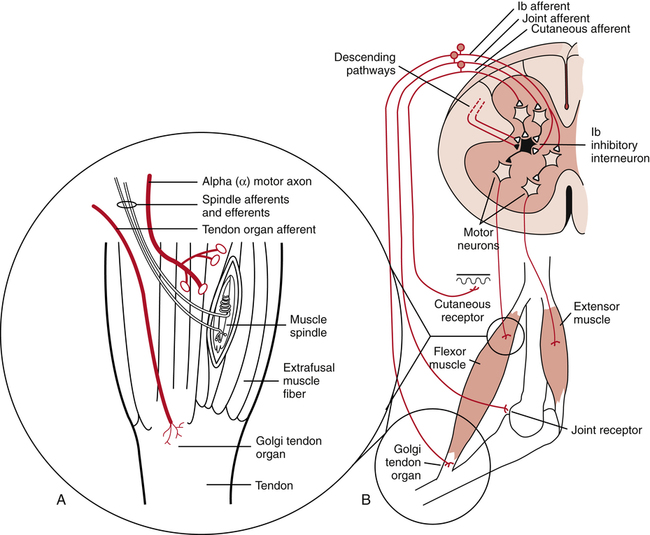
On the other hand, many researchers suggest that the immediate result of stretching is attributed to neurophysiologic phenomena.69 They categorize these phenomena as either a stretch tolerance or active contractile responses and claim that the limiting factor during stretching is the muscular resistance secondary to reflex activity. A stretch tolerance simply means an accommodation to the discomfort of stretching over time. With this philosophy, the aim of stretching is to inhibit the reflex activity, subsequently decreasing the resistance and improving ROM. Several other researchers agree and recommend certain types of stretching for its reduction in reflex activity.3,43,50 Muscle spindles and Golgi tendon organs are the mechanoreceptors responsible for the contractile responses (Fig 3-10).
Warm-up
Warm-up is necessary to help prepare the tissue for activity. Stretching alone before exercise is not recommended by most researchers and health professionals.65,66,111,124 As such, the purpose of warm-up exercises, including stretching, is to prepare the body for the stresses it will encounter during an activity or sport and is necessary for increasing the core body temperature. Heat is produced with muscle contraction, thereby increasing the intramuscular temperature.23 ROM increases as a result of warmed tissue.107 A warmed muscle will be able to contract more forcefully and relax more quickly,15 thereby enhancing work production for those muscles used.16 In training, a general body warm-up is needed first. The beneficial effects of a warm-up before strenuous activities include the following:
 Blood flow to working muscles is increased.
Blood flow to working muscles is increased.
 Temperature in working muscles is increased.
Temperature in working muscles is increased.
 Cardiovascular response to sudden, dynamic exercise is improved.
Cardiovascular response to sudden, dynamic exercise is improved.
 Breakdown of oxyhemoglobin for the delivery of oxygen to the working muscles is increased.
Breakdown of oxyhemoglobin for the delivery of oxygen to the working muscles is increased.
With warm-up, the risk of connective tissue and contractile tissue damage is reduced. Warm-up protocols usually last from 10 to 25 minutes or more and may vary somewhat, depending on the nature of the activity or event.8 The warm-up should be intense enough to cause an increase in body temperature, but not so intense as to cause fatigue. So one should taper the warm-up 5 to 10 minutes before the actual event.3 It is clinically assumed, of course, that a more compliant muscle can be stretched further and is therefore less susceptible to injury.48
However, some think that the warm-up period may not be the best time to stretch for increasing ROM, primarily because of increased tissue stiffness. Since the concept of stretching to prevent injury has come under question, benefits of stretching before activity may be incorrect. Activity of gradually increasing intensity (dynamic stretching) may be more appropriate than static stretching as a warm-up activity.96 Some researchers have examined the combination of stretching and active warm-up and have shown that the decrease in stiffness mainly results from increased muscle temperature and not stretching.85,104
Increasing intramuscular temperature to help increase ROM may also be achieved through external means.110 Henricson and colleagues57 reported on results that followed the application of heat to the hip. Although heat alone did not improve hip ROM, stretching without heat did increase hip ROM, and stretching with heat combined gave the greatest increase in ROM, maintaining it for 30 minutes. These results are consistent with others,62,74,127 who report that collagen extensibility increases and musculotendinous stiffness decreases with heat. Bear in mind, however, that most authors recommend using exercise as the primary way of increasing intramuscular temperature.96 It has not been definitively shown whether a general warm-up serves to improve sports performance.17,18,21,46
Stretching Techniques
In discussion of flexibility and associated stretching programs, the stretching of nonpathologic muscle must be separated from stretching noncontractile connective tissue. Improving muscle extensibility in nonpathologic conditions and in adaptive muscle shortening after injury or immobilization requires a complement of active exercise techniques and thermal agents. Types of stretching exercises are static stretching (active and passive), ballistic stretching, dynamic stretching, and proprioceptive neuromuscular facilitation (PNF) techniques (contract-relax, contract-relax with agonist contraction, and hold-relax). Research has shown that all four techniques have been shown to increase flexibility.31,56,61,80,82,105 Essential to a successful stretching program for improving flexibility is the proper execution of the exercises.
Static stretching
The most common form of stretching exercise that is used to safely increase the ROM in a joint is static stretching. This form of stretching allows one to sustain a controlled stretch by placing a muscle in a fully elongated position and holding that position for a period of time (Fig. 3-11




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


