22
Orthopedic Management of the Elbow
1. Identify and describe the principles for common overuse and soft-tissue injuries of the elbow.
2. Discuss common methods of management and rehabilitation of overuse, soft-tissue injuries of the elbow.
3. Identify and describe intercondylar fractures, radial head fractures, olecranon fractures, and fracture-dislocations of the elbow.
4. Describe methods of management and rehabilitation of various fractures and fracture-dislocations of the elbow.
5. Describe techniques to improve range of motion of a stiff elbow including common joint mobilization techniques.
SOFT-TISSUE INJURIES OF THE ELBOW
Lateral Epicondylitis
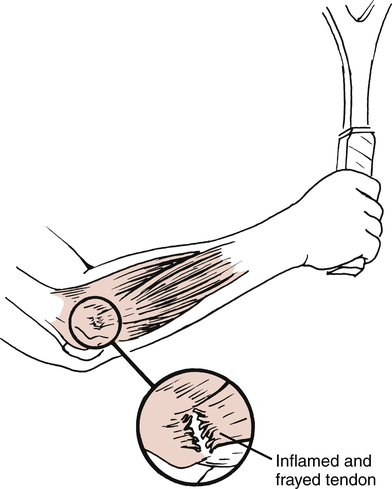
Commonly referred to as tennis elbow, lateral epicondylitis affects the common wrist extensor origin of the extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi.8,29 The repetitive overuse of this area leads to tendinitis of the origin of the extensor carpi radialis brevis tendon (Fig. 22-1).9,29
Interestingly, lateral epicondylitis can affect anyone involved with repetitive activities of the wrist extensors.28 Thus persons involved with the use of hand tools (e.g., hammer, screwdriver, or pliers) and various activities involving wrist rotation, pulling, extending, and hand grasping can be affected by lateral epicondylitis.28
Generally the patient suffering from lateral epicondylitis has pain with palpation of the lateral epicondyle, with active or resisted wrist extension, and occasionally with grasping of the affected hand.8,23,28 Because this is a chronic overuse tendinitis, the intense inflammatory response in the affected area of the lateral epicondyle is “an attempt to increase the rate of tissue production to compensate for the increased rate of tissue microdamage.”28
Management of Lateral Epicondylitis
Initial acute management focuses on resolving pain and swelling with the judicious use of ice massage directly over the affected area, phonophoresis or iontophoresis, physician-prescribed analgesics and nonsteroidal antiinflammatory drugs (NSAIDs), rest, and protection of the area from unwanted stress to allow for healing.8,23,28
Relative rest rather than strict immobilization is used. A wrist cock-up splint can be used in severe cases to minimize stress on the inflamed wrist extensor tendons. The patient is allowed to remove the splint as needed to participate in controlled motion exercises that do not produce pain. Long-term, rigid immobilization is not indicated, because treatment goals are to not only reduce pain and swelling but also to encourage proper collagen alignment and scar tissue maturation.23 Without early protected motion, excessive tissue scarring and random collagen fiber alignment would severely limit normalized motion and function of the elbow and wrist.
During the initial healing stage, the PTA must encourage the patient to avoid any and all motions that may adversely affect healing. Short-term modifications in activities of daily living (ADLs), sports, and job-related activities must be addressed to provide a pain-free environment for healing. When this initial program fails to bring significant relief of symptoms, some physicians elect to inject the area with a steroid to reduce the inflammation.20,23
In addition, active gentle static stretching is advised for the wrist extensors to produce normalized, pain-free wrist flexion and extension (Fig. 22-2). Although specifically addressing treatment for the elbow, active motion and resistance exercises for the elbow and shoulder can be initiated if no wrist motion occurs to increase symptoms.

The PTA must carefully instruct the patient to perform all exercises within a pain-free range of motion (ROM). Throughout all phases of recovery, the patient must avoid stressful, pain-producing activities to prevent the exacerbation of the inflammatory condition. Progressive motion exercises and increased resistance exercise are the foundation for a return to functional activities. Concentric and eccentric muscle contractions are added once the patient can demonstrate increased quality of multiangle isometric contractions. Care must be taken when initiating both concentric and eccentric resistance exercises because frequently these contractions produce symptoms. Light resistance is advocated when having patients perform these exercises for the first time. An important component for all resistance exercises used with lateral epicondylitis is the performance of slow, controlled eccentric contractions. Eccentric muscle contractions produce greater tension than either concentric or isometric exercise. In addition, energy use involving adenosine triphosphate (ATP) is less for eccentric exercise than for either concentric or isometric exercise. Eccentric muscle contractions are, in fact, advocated by Curwin and Stanish8 for the treatment of tennis elbow, and the rationale for the performance of eccentric exercise is described by Reid and Kushner24 as, “Exercising the muscle eccentrically allows it to withstand greater resistance and prevent injury, which occurs by eccentrically loading an inflexible muscle.”24
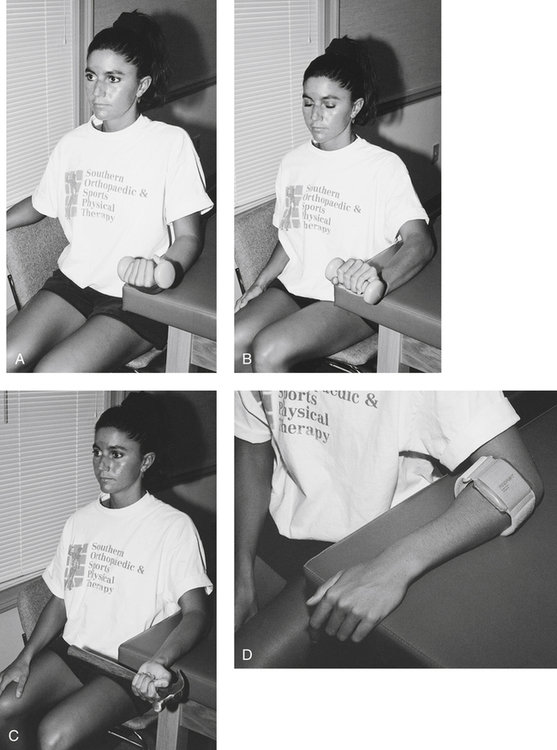
Resistive exercises emphasizing the eccentric phase are described in Figure 22-3, A-B. A hammer is an effective strengthening tool for the treatment of lateral epicondylitis. However, when instructing the patient to perform pronation and supination of the forearm for the first time, the PTA should have the patient hold the hammer close to its head (Fig. 22-3, C). As the patient gains strength and can control the resistance of the hammer eccentrically, the patient should gradually hold the hammer at the midshaft. As strength improves further, the patient should be allowed to hold the hammer at the end of the shaft, which requires greater eccentric muscle control, strength, and torque. In the same manner, strength can be gained for radial and ulnar deviation through use of the hammer. With a gradual return to functional activities, some physicians and therapists advocate the use of a counterforce brace to help dissipate the “overload forces” on the common origin of the wrist extensors (Fig. 22-3, D).8,20,28
Surgery is rarely necessary for this condition because physical therapy management frequently is effective. In rare instances when conservative means fail to reduce pain and improve function, the surgeon may elect to surgically excise the “angiofibroblastic tissue at the origin of the extensor carpi radialis brevis muscle.”29
Medial Epicondylitis
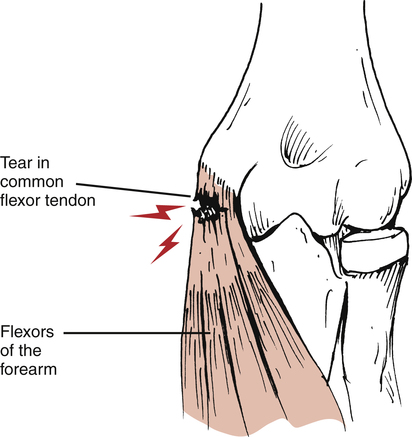
Medial epicondylitis, an overuse condition, affects the origin of the pronator teres, flexor carpi radialis, flexor digitorum sublimis, and flexor carpi ulnaris at the medial epicondyle of the elbow.23 Although it occurs less often than lateral epicondylitis (the ratio of lateral epicondylitis to medial epicondylitis is 7:1),28 it is no less incapacitating to the patient. Again the dominant feature is pain with palpation over the medial epicondyle, active motion, and particularly with resisted wrist flexion and full passive wrist extension (Fig. 22-4).23,24
Management of Medial Epicondylitis
The acute management phase of this inflammatory overuse condition, also referred to as golfer’s elbow, concentrates on the management of pain and swelling. Usually the physician prescribes NSAIDs, ice (protect the ulnar nerve), phonophoresis or iontophoresis, relative active rest (not immobilization), protection, and gentle active motion exercises. The criteria-based treatment plan parallels that for lateral epicondylitis, although it obviously focuses on the wrist flexors. Static low-load, long-duration stretching3,4 can proceed as pain allows. The PTA must encourage the patient to avoid repetitive flexing of the wrist and pronating of the forearm if these motions produce pain. Modifications in lifting, twisting, pulling, or turning of the wrist and forearm must accompany each phase of recovery to avoid stress on the medial structures. Moist heat and ultrasound can be applied to the medial epicondyle before stretching once motion has improved without pain. Resistance training can then begin with submaximal isometrics, progressing to higher-quality isometric multiangle contractions, and ultimately to concentric and eccentric isotonic and isokinetic resistance exercises. The patient is instructed in the active use of the shoulder of the affected limb and strongly encouraged to follow a conditioning program to maintain or enhance cardiovascular fitness, strength, and flexibility throughout the rehabilitation process.
Although the resolution of pain and swelling is paramount for active use of the wrist and forearm, regaining lost motion caused by pain and muscular dysfunction is critical for function and a return to normal daily activities. The normal elbow ROM is 0° to approximately 145° of flexion.29 However, most daily activities can be carried out within a functional ROM of 30° to 130° of flexion.24,29 In addition, normal pronation of 75° and supination of 85° exceeds the functional arc of motion of 50° needed to carry out most ADLs. Therefore the PTA must encourage pain-free early protected motion to facilitate the collagen fiber alignment needed for both functional scar maturation and purposeful motion to perform ADLs.
Medial Valgus Stress Overload
Injuries to the elbow often occur in the overhead athlete. The repetitive overhead motion involved in throwing is responsible for unique and sport-specific patterns of injuries to the elbow. These are caused by chronic stress overload or repetitive micro-traumatic stress observed during the overhead pitching motion as the elbow extends at over 2300°/s, producing a medial shear force of 300 N and lateral compressive force of 900 N.11,32 In addition, the valgus stress applied to the elbow during the acceleration phase of throwing is 64 N·m,11,32 which exceeds the ultimate tensile strength of the ulnar collateral ligament.10 Thus the medial aspect of the elbow undergoes tremendous tensile (distraction) forces and the lateral aspect is forcefully compressed during the throwing motion.
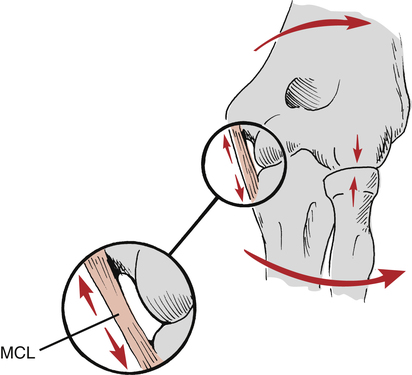
Medial valgus stress overload, also known as valgus extension overload (VEO) occurs commonly among patients who participate in repetitive throwing and racquet sports such as javelin throwing, baseball, racquetball, and tennis.9,21,23 The overhead athlete is susceptible to these specific elbow injuries. A number of forces act on the elbow during the act of throwing,11,32 including valgus stress with tension across the medial aspect of the elbow. These forces are maximal during the acceleration phase of throwing. Compression forces are also applied to the lateral aspect of the elbow during the throwing motion. The posterior compartment is subject to tensile, compressive, and torsional forces during acceleration and deceleration phases. This may result in valgus extension overload within the posterior compartment, leading to osteophyte formation, stress fractures of the olecranon, or physeal injury.1,35 These stresses approach the ultimate failure load of the ligament with each throw. The repetitive nature of overhead throwing activities such as baseball pitching, javelin throwing, and football passing further increase the susceptibility of medial elbow injuries including ulnar collateral ligament (UCL) injuries, by exposing the ligament to repetitive micro-traumatic forces. Clinical differences exist between medial valgus stress overload and medial epicondylitis. Although medial epicondylitis represents a chronic overuse syndrome affecting the soft-tissue musculotendinous origin of the wrist flexors and pronators, medial valgus stress overload occurs to the capsuloligamentous structures (medial [ulnar] collateral ligament) as a result of repetitive valgus stress to the elbow (Fig. 22-5).9,21,23
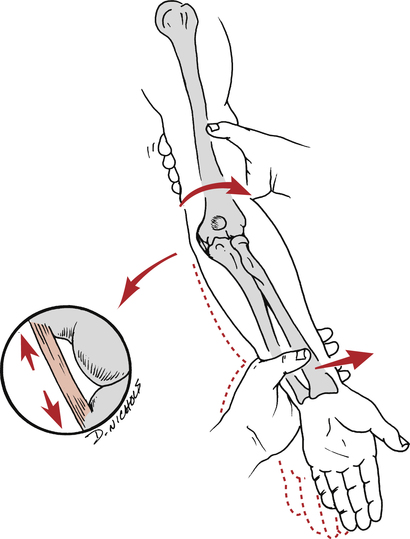
Patients usually complain of pain over the medial aspect of the elbow and the posterior aspect of the olecranon.21,23 During the physical therapist’s (PT) initial evaluation, the PTA may observe the performance of ligament stability tests to confirm the presence of UCL laxity. The affected arm is held in 20° to 30° of flexion while the humerus is held in full external rotation to unlock the olecranon process from the olecranon fossa. A medial or valgus stress then is applied to the elbow to assess the stability of the UCL (Fig. 22-6).21,23
Management of Medial Valgus Stress Overload
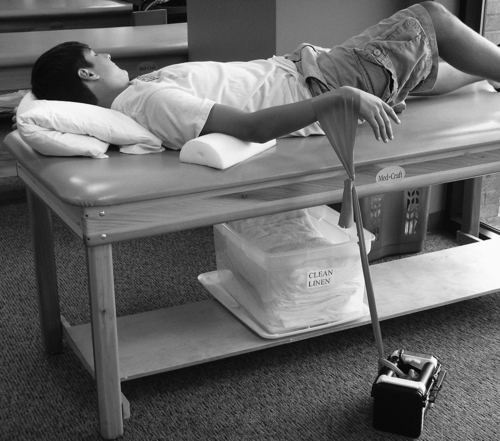
The elbow is predisposed to flexion contractures due to the intimate congruency of the joint articulations, the tightness of the joint capsule, and the tendency of the anterior capsule to develop adhesions following injury.33 The brachialis muscle also attaches to the capsule and crosses the elbow joint before becoming a tendinous structure. Injury to the elbow may cause excessive scar tissue formation of the brachialis muscle as well as functional splinting of the elbow.33 Gentle low-load static stretching begins as soon as pain allows. Therefore the stretching regimen focuses on all wrist motions, forearm pronation and supination, and elbow flexion and extension as long as no symptoms of pain occur with these activities. If the patient continues to have difficulty achieving full extension using ROM and mobilization techniques, a low-load, long duration (LLLD) stretch may be performed to produce a deformation (creep) of the collagen tissue, resulting in tissue elongation.12,27,30,31 This technique is extremely beneficial for regaining full elbow extension. The patient lies supine with a towel roll or foam placed under the distal brachium to act as a cushion and fulcrum. Light resistance exercise tubing is applied to the wrist of the patient and secured to the table or a dumbbell on the ground (Fig. 22-7). The patient is instructed to relax as much as possible for 10 to 15 minutes per treatment. The amount of resistance applied should be of low magnitude to enable the patient to perform the stretch for the entire duration without pain or muscle spasm. This technique should impart a LLLD over a prolonged period of time to achieve maximal benefits. Patients are instructed to perform this stretch technique several times per day, equaling 60 minutes of total end range time. Patients may perform a 15 minute stretch, 4 times per day.16 This program has been extremely beneficial for patients with a stiff elbow.
Surgery is considered if conservative treatment fails to restore function and eliminate pain. Degenerative changes, which are usually present in the adult, must be addressed surgically.21,24 In general, an osteotomy is performed to remove osteophytes (bone spurs) and fibrotic, degenerated tissue.21,24
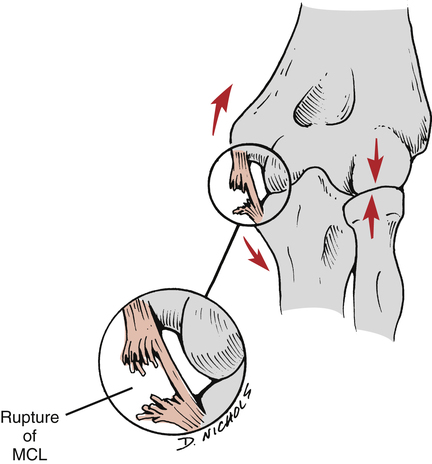
Acute rupture (grade III ligament rupture) of the medial (ulnar) collateral ligament can occur in skeletally mature adults if valgus stress is applied suddenly with sufficient force (Fig. 22-8).
If early active protected joint motion and progressive resistance exercise have been used, authorities suggest that the injured patient can resume throwing activities approximately 3 months after injury.21 However, surgery may be necessary to stabilize the joint if the patient does not demonstrate improved valgus stability and continues to have dysfunction.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


