26
Introduction to Orthotics and Prosthetics
1. Define the terms orthotics and prosthetics.
2. Obtain basic understanding of materials.
3. Learn the nomenclature—the naming of orthoses and prostheses in relation to the joint they support or replace.
4. Describe the key differences when off-the-shelf orthoses can be chosen instead of custom fabricated.
5. Have a general understanding of orthotic options for supporting major joints in the body.
6. List levels of amputation sites as well as the reasons for amputation.
7. Develop an understanding of basic prosthetic componentry and how the selection of componentry relates to patient function and outcome.
The process developed for naming orthoses and prostheses is a fairly simple technique. The International Standards Organization (ISO) recognizes common descriptors for orthoses and prostheses, based on the acronyms from the body joint or joints that are supported or replaced (Table 26-1). This method of nomenclature is both effective and easily learned.
Table 26-1
ISO Naming Conventions for Orthoses and Prostheses
| Device Type | Amputation Level | Nomenclature | |
| Orthoses | Upper extremity | Finger orthosis | FO |
| Hand orthosis | HO | ||
| Wrist-hand orthosis | WHO | ||
| Wrist orthosis | WO | ||
| Elbow orthosis | EO | ||
| Elbow-wrist-hand orthosis | EWHO | ||
| Shoulder orthosis | SO | ||
| Spinal | Cervical-thoracic-lumbosacral orthosis | CTLSO | |
| Cervical orthosis | CO | ||
| Thoracic-lumbosacral orthosis | TLSO | ||
| Lumbosacral orthosis | LSO | ||
| Sacroiliac orthosis | SIO | ||
| Lower extremity | Foot orthosis | FO | |
| Knee orthosis | KO | ||
| Ankle-foot orthosis | AFO | ||
| Knee-ankle-foot orthosis | KAFO | ||
| Hip-knee-ankle-foot orthosis | HKAFO | ||
| Prostheses | Upper extremity | Shoulder disarticulation | SD |
| Trans-humeral | TH | ||
| Elbow disarticulation | ED | ||
| Trans-radial | TR | ||
| Wrist disarticulation | WD | ||
| Lower extremity | Hip disarticulation | HD | |
| Trans-femoral | TF | ||
| Knee disarticulation | KD | ||
| Trans-tibial | TT | ||
| Ankle disarticulation | Symes | ||
| Trans-metatarsal amputation | TMA | ||
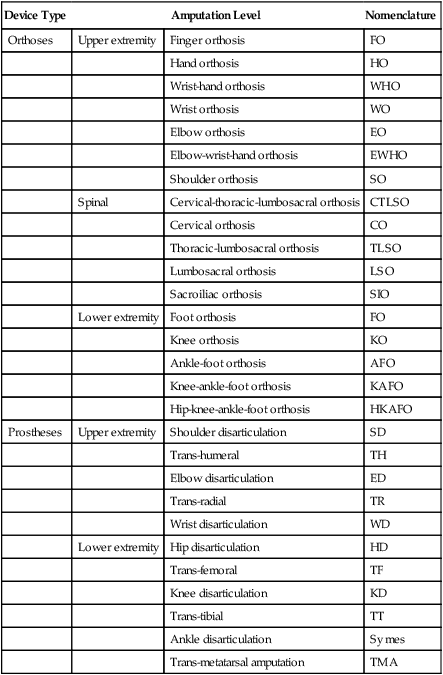
From Shurr DG, Michael JW: Prosthetics and orthotics, ed 2, Upper Saddle River, NJ, 2002, Prentice Hall, p 16.
PROSTHETICS
A prosthesis is any device that replaces a body part. This group consists of arms, legs, partial feet, hands, ears, breasts, and so on. The goal for each prosthesis is to provide function, body balance, ease of use, and optimal cosmesis in order to restore self image, quality of life, and independence (Table 26-2). Prostheses are custom fabricated and require adjustments and realignment on a regular basis.
Table 26-2
Specifications for the Ideal Prosthesis/Orthosis
| Need | Definition |
| Function | Meets the user’s needs, simple, easily learned, dependable |
| Comfort | Fits well, easy to don/doff, lightweight, adjustable |
| Cosmesis | Looks, smells, sounds “normal,” cleans easily, stain-resistant |
| Fabrication | Fast, modular, readily and widely available |
| Economics | Affordable, worth cost of monetary investment |
From Shurr DG, Michael JW: Prosthetics and orthotics, ed 2, Upper Saddle River, NJ, 2002, Prentice Hall, p 29.
Fitting for Orthoses or Prostheses
Material Selection
When fabricating orthoses and prostheses, the material selection is the first consideration of the process. There are multiple types of thermoplastics, metals, carbon fiber composites, and interface materials to choose from. Each type of material will have certain desirable characteristics or properties that will best suit each patient’s needs. Body weight, activity level, amount of rigidity needed, flexibility of material, energy storing properties, amount of cushioning required, and patient strength are all variables to consider when selecting fabrication materials (Table 26-3).
Table 26-3
Important Characteristics of Prosthetic and Orthotic Materials
| Need | Definition |
| Strength | Maximum external load that can be withstood |
| Stiffness | Stress/strain or force-to-displacement ratio |
| Durability | Ability to withstand repeated loading |
| Density | Weight per unit volume |
| Corrosion resistance | Resistance to chemical degradation |
| Ease of fabrication | Equipment and techniques needed to shape it |
From Shurr DG, Michael JW: Prosthetics and orthotics, ed 2, Upper Saddle River, NJ, 2002, Prentice Hall, p 29.
DEVICE SELECTION
Orthoses
Upper Extremity
Fingers, hand, and wrist
A splint for the fingers and hand should only support the affected joint or joints and allow the unaffected joints free ROM. There are single joint splints for the fingers available, such as proximal interphalangeal (PIP) and distal interphalangeal (DIP) splints which maintain or promote active range of motion (AROM) in the phalanges after sprains, fractures, or contractures. Some splints maintain or hold the joint in a fixed position, whereas dynamic splints that are spring-loaded allow the patient some movement of flexion or extension while applying constant force in the desired direction (Fig. 26-1). One particular type of wrist-hand-finger orthosis (WHFO) is the Thomas suspension splint. The function of this splint is to apply tension to the wrist joint and thumb in order to dorsiflex the wrist for diagnoses such as radial palsy. The long opponens splint is often used for flexion contractures, nerve or tendon damage due to traumatic accidents, or rheumatoid arthritis. These splints offer dynamic finger extension and allow the patient to use flexors needed for gripping.

Another example of a functional custom fabricated WHFO is the tenodesis splint (also known as a wrist action splint) (Fig. 26-2). This splint is used to increase functional levels and independence mainly for quadriplegia. The design is ultra lightweight and uses the available ability to flex the wrist to accentuate the natural movement of opposition for gripping objects by using the three-jaw chuck pinch position. The wrist-driven wrist/hand orthosis employs the flexor hinge principle. The fingers and thumb are stabilized in the position of function. A small amount of wrist extensor strength will create flexion motion in the metacarpal phalangeal (MP) joints to produce adequate pinch for a variety of daily activities. Because it is custom fabricated, this style of splint requires a cast of the hand and forearm and measurements for fabrication.

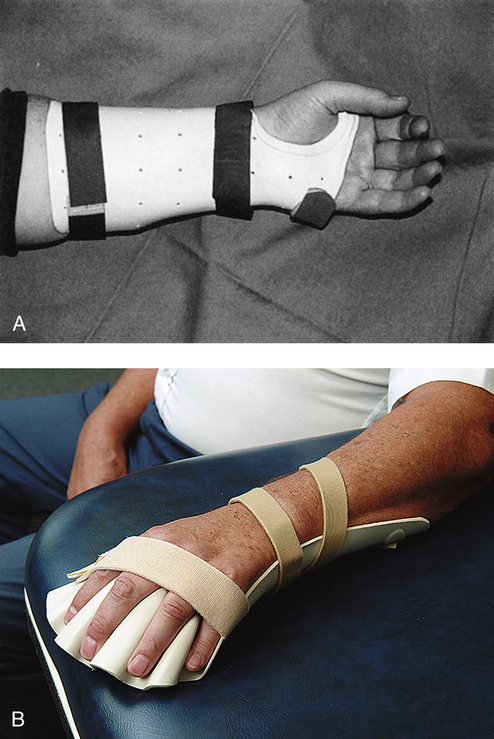
There are multiple orthotic options available when supporting the hand and wrist, depending on the diagnosis and desired limitations for movement. For diagnoses such as carpal tunnel syndrome, tendonitis, or a sprain, a cock-up wrist splint, which holds the wrist in a neutral position is the most common choice (Fig. 26-3, A). This splint is a prefabricated brace that is readily available in varying sizes. For diagnoses such as a contracture secondary to a cerebral vascular accident (CVA) or rheumatoid arthritis (RA), a prefabricated malleable wrist-hand-finger orthosis will suffice. This orthosis is progressive in design because the wrist joint and finger platform is easily flexed or extended to accommodate gains made by stretching protocols in physical therapy sessions. These prefabricated, lightweight splints are called platform or resting splints and provide static positioning (Fig. 26-3, B). Some of the soft versions of these splints are more skin-friendly because they offer the option of a cover that can be removed and washed, which promotes good hygiene.
Elbow
Fitting choices for elbow orthoses can usually be prefabricated. A lateral epicondylitis splint (a band with a silicone or air pocket), is used to disperse the pressure placed on the tendon caused by use over a greater area, thus decreasing the point of high stress and pain (Fig. 26-4). ROM splints that limit AROM or provide pressure to increase ROM can also be purchased as prefabricated orthoses. The Flex POP Elbow Orthosis by RCAI (St. Petersburg, Fla.), for example, provides rehabilitation for joint stiffness and contractures, instabilities, strains, sprains, and ligament repairs. This ROM elbow orthosis offers flexion/extension stop sets at 5-degree increments, which allows changes to be made in therapy sessions as the patient progresses. Dynamic elbow splints can be used when the function desired is to gain ROM by applying a constant stretch to the elbow joint tendons and muscles. Protocols are set for wear time and when the tension placed upon the joint can be increased. Static splints can be set to a designated degree of flexion or extension and depending upon the style or brand, may or may not be adjustable. The physician’s prescription, rehabilitation protocols, and the patient’s level of compliance and tolerance all contribute to the decision-making process when fitting these types of elbow splints. Elbow contractures can be caused by a variety of injuries or diseases, such as cerebral palsy and CVA.

Shoulder
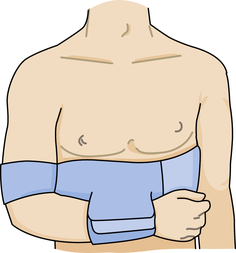
Shoulder splinting for immobilization can use a sling and swath or a shoulder immobilizer that will support the shoulder joint. One commonly used design utilizes a chest band, upper arm cuff, and a forearm cuff that is adjustable and positions the arm securely against the body (Fig. 26-5). If the required position is abduction, then an airplane splint can be fitted.
Specialized orthoses for the upper extremity
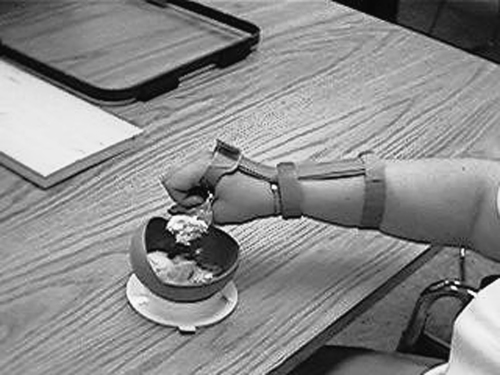
ADLs require a multitude of orthoses to promote independence for individuals who have suffered a stroke or debilitating injury. There are hand and wrist splints that are used to assist with feeding oneself, holding an ink pen, using a brush, and so on (Fig. 26-6). There are many types of foam available to place around utensils and items with handles to increase their circumference, therefore decreasing the grip strength and ROM needed to hold and use such items.
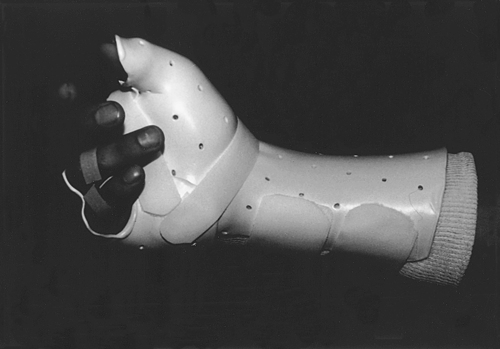
Fracture splinting uses a compression method for stabilization of the fracture site. The compression of fluid and soft tissue around the fracture site is key when providing a femoral, humeral, radial, or ulnar splint. These splints can be modified to a custom fit by heating and/or adding a soft interface material to provide added comfort. The fracture splint is a bivalve, two-piece orthosis and uses adjustable hook and loop strapping (Fig. 26-7). The splint will allow movement of the unaffected joints such as elbow and wrist for the ulnar fracture. The technique and principles used in splinting for upper extremity fractures is the same for lower extremity fractures.
Spine and Trunk
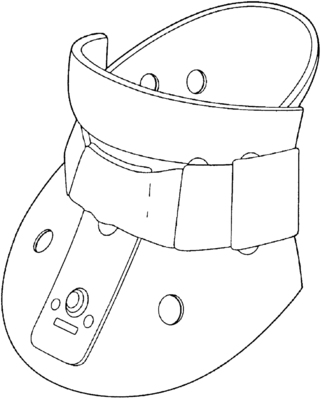
Cervical spine
Cervical orthoses are fitted for the purpose of supporting the cervical muscles; limiting rotation, flexion, and extension; or immobilization of the cervical spine. A soft cervical collar can be fitted for lesser injuries such as sprains and strains. The soft collar is a prefabricated orthosis made of foam with a cotton cover and has a hook and loop closure in the back (Fig. 26-8). They are available in different heights and lengths. A cervicothoracic orthosis is a semirigid, two-piece brace that can be fitted for whiplash, degenerative joint disease, arthritis, and presurgical or postsurgical repairs. These collars are adjustable in height, circumference, and rigidity, but, as with all bracing, the therapist must always check pressure points to make sure that there is no skin breakdown.