Femur
Joseph R. Cass
ANTEROMEDIAL APPROACH TO THE FEMUR
Indications
Situations in which combined exposure of the knee and femoral shaft is necessary, such as for the placement of large revision knee arthroplasty components.
Extension
The exposure can be extended distally to complete a medial parapatellar approach to the knee. Proximal extension is limited by the femoral artery crossing the wound.
Anatomy
The anteromedial approach is distant from any important neurovascular structures and it involves a transmuscular plane to the femur. This approach to the femur is performed between the vastus medialis and rectus femoris in the superficial layer and involves splitting the vastus intermedius in the deep layer to access the femur.
Technique
Incision: if it is possible to determine the location of the medial border of the vastus medialis the incision should follow this contour, extending proximally from a point just proximal and medial to the superomedial pole of the patella. If the vastus medialis contour is unable to be determined, the incision should be carried in a longitudinal fashion from a point medial and proximal to the superomedial pole of the patella (Fig. 8-1).
The deep fascia of the thigh is incised in line with the skin incision and flaps are elevated medially and laterally (Fig. 8-2). The interval between the vastus medialis and rectus femoris is identified and is developed with blunt dissection proximally.
As this interval is continued distally, the quadriceps tendon is incised close to its medial border, leaving adequate amount of tendon medially and laterally for later closure (Fig. 8-3).
Deep to the vastus medialis and rectus femoris, the vastus intermedius is split in line with its fibers (Fig. 8-4).
Subperiosteal dissection along the femoral shaft elevates the vastus intermedius off the femur (Fig. 8-5). Retraction of the vastus medialis in the lateral and medial direction allows complete exposure of the anterior aspect of the distal femur.
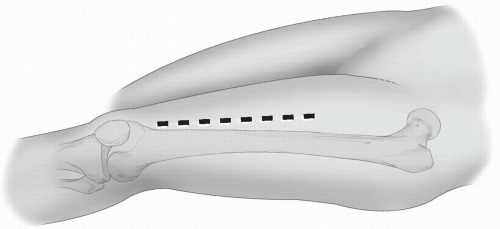 FIGURE 8-1 The skin incision typically extends proximally as needed from a point just medial and superior to the superomedial aspect of the patella. |
Closure
Muscle reapproximation of the vastus intermedius is not possible. Closure consists of first repairing the incision in the quadriceps tendon, followed by reapproximating the deep fascia.
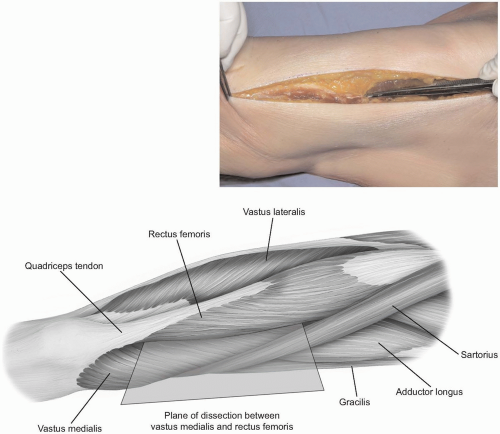 FIGURE 8-2 The deep fascia of the thigh is split to expose the interval between the vastus medialis and rectus femoris. Distally, the muscles join to form the quadriceps tendon. |
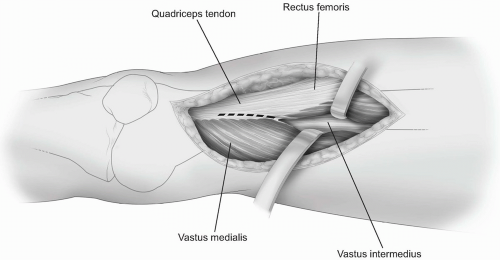 FIGURE 8-3 The interval between the vastus medialis and rectus femoris is developed with blunt dissection. Distally, the quadriceps tendon may need to be split in order to access the distal femur and articular surface. |
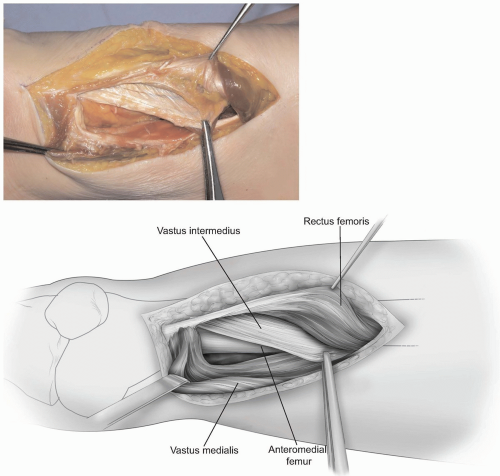 FIGURE 8-4 The vastus intermedius is deep to the interval developed. |
 FIGURE 8-5 Subperiosteal dissection of the vastus intermedius medially and laterally allows exposure of the anterior femur. |
ANTEROLATERAL APPROACH TO THE FEMUR
Indications
Fractures, bone grafting, total femoral replacement, and extensor mechanism repair.
Extension
The exposure can be extended proximally to expose the hip joint and distally to expose the knee joint through a lateral parapatellar approach.
Anatomy
The interval between the rectus femoris and vastus lateralis is developed in order to expose the vastus intermedius. The approach involves splitting the fibers of the vastus intermedius to access the femoral shaft. The descending branch of the lateral femoral circumflex artery crosses the plane between the rectus femoris and the vastus lateralis in the proximal thigh. The artery enters the vastus lateralis along with the motor branch of the nerve to the vastus lateralis and should be preserved as it enters the vastus lateralis. A branch of the vessel continues along the medial side of the vastus lateralis to join the arterial anastomosis around the knee.
Technique
Incision: the incision is made along a line from the anterior-superior iliac spine to the lateral aspect of the patella. The length of the incision is determined by the pathology being addressed. The skin and subcutaneous tissue are incised in the line described (Fig. 8-6) to expose the deep fascia of the thigh.
The fascia is split in line with the skin incision and the interval between the rectus femoris and vastus lateralis is identified (Fig. 8-7).
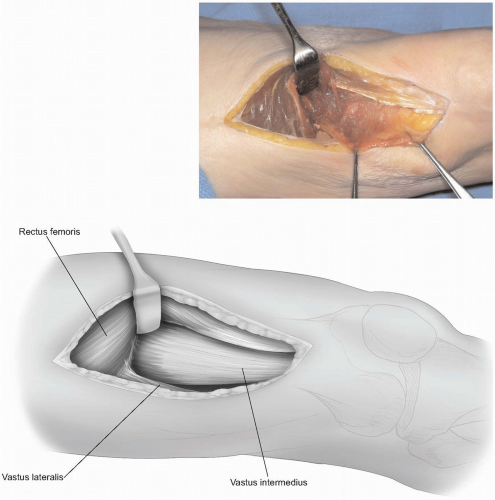
This interval is easily developed in the middle of the thigh. In the distal thigh, the muscles are adherent, connected by an aponeurotic sheet of tissue. This connection will need to be split in order to access the vastus intermedius in the distal thigh (Fig. 8-8). Proximally, care should be taken in order to prevent injury to the descending branch of the lateral femoral circumflex artery and motor nerve to the vastus lateralis as they cross from the rectus femoris to the vastus lateralis together.
The vastus intermedius muscle belly is split in line with its fibers to expose the anterior femoral shaft. Subperiosteal dissection medially and laterally to elevate the vastus intermedius will further expose the anterior aspect of the femur (Fig. 8-9).
 FIGURE 8-6 The skin incision is made along a line connecting the anterior-superior iliac spine and the lateral edge of the patella. The location of the incision along this line depends on the region of the femur that needs to be exposed. |
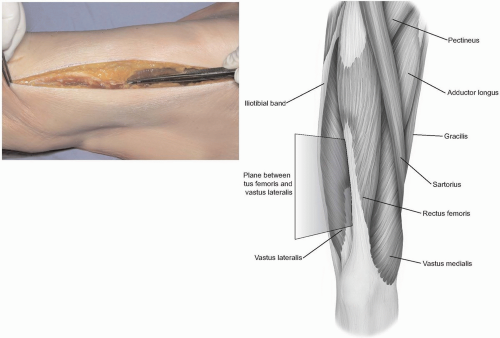 FIGURE 8-7 The deep fascia of the thigh is split in line with the skin incision and the rectus femoris and vastus lateralis muscles are identified. |
Closure
Muscle reapproximation of the vastus intermedius is not possible. Closure consists of reapproximating the deep fascia followed by routine subcutaneous tissue and skin closures.
POSTEROLATERAL APPROACH TO THE FEMUR
Indications
Reduction and internal fixation of femoral shaft fractures, subtrochanteric and intertrochanteric fractures, and biopsy and treatment of bone tumors.
Extension
The posterolateral approach to the femur can be extended proximally and combined with multiple hip exposures to expose the proximal femur. Distally, the exposure is easily extended to a lateral parapatellar approach to the knee joint.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





