FIGURE 21-1. A: Radiograph of failed Austin Moore type implant in elderly patient. The remaining cancellous bone is good. B: Radiograph after revision with cemented stem. Note the goodquality bone-cement interface.
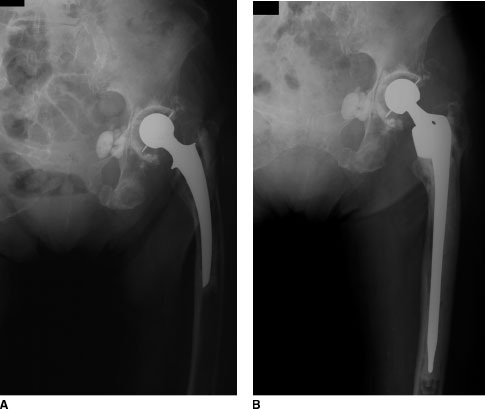
FIGURE 21-2. A: Radiograph of failed total hip arthroplasty in elderly patient with poor-quality bone. B: Radiograph after revision with cemented long-stem implant. The long-stem gains cement purchase in fresh cancellous bone.
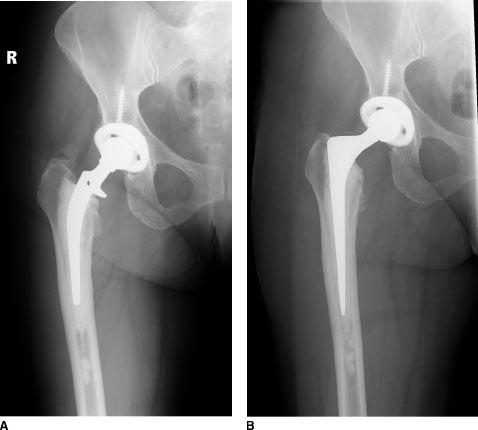
FIGURE 21-3. A: Radiograph of failed total hip arthroplasty with debonded stem (at prosthesis-cement interface) but good cement mantle with intact bone-cement interface. B: Radiograph after revision using cement-in-cement technique with tapered polished stem.
Proximally Porous-Coated Uncemented Implants Unitized Femoral Components. Unitized, tapered, proximally porous-coated, uncemented implants have lost favor for femoral revision. Poor results associated with this method are attributable to the limited uncemented fixation surface area which is applied to poor quality, weak, sclerotic, avascular bone in the proximal femur (Fig. 21-4).20 Furthermore, it is difficult to shape the proximal femur with broaches to gain intimate bone contact between the prosthesis and the bone.

FIGURE 21-4. Immediate postrevision (left) and follow-up (right) radiographs showing failure of proximally porous-coated nonmodular stemmed implant for revision THA. Implants of this general category had a poor track record of bone ingrowth and a high failure rate.
Proximally Porous-Coated Modular Implants. Proximally porous-coated modular implants continue to play a valuable role in revision surgery, particularly when sufficient proximal bone stock is present to allow a proximally fixed implant to gain immediate- and long-term fixation.21–24 Most surgeons do not favor these implants when proximal bone loss is marked, or when an extended osteotomy will be performed. Modern modular implants allow milling of the proximal femur to expose good remaining bone, and provide intimate prosthesis-bone contact based on optimal sizing provided by implant modularity. Most of these implants have a fluted, distal section that provides extra early stability from diaphyseal fit. These implants are discussed in more detail in Chapter 23 (Fig. 21-5).

FIGURE 21-5. Radiograph after successful revision with modular proximally coated uncemented stem.
Proximally Coated Calcar-Replacing Implants These implants gain rotational control and bone ingrowth in the metaphyseal-diaphyseal region, and axial stability from a calcar-replacing platform. Favorable midterm results have been reported.25 Most proponents use extensively porous-coated versions of these implants, or other alternatives, when proximal bone loss is marked. These implants are discussed in more detail in Chapter 24 (Fig. 21-6).

FIGURE 21-6. Radiograph demonstrating well-fixed proximally coated calcar-replacing stem after revision total hip arthroplasty
Uncemented Extensively Coated Parallel-Sided Implants These implants include both extensively porous-coated implants, rough grit-blasted parallel-sided implants (of either a tapered or calcar-replacing type design), and hydroxyapatite-coated implants (Figs. 21-7 and 21-8). Because these implants gain stability in the diaphysis, they are versatile and applicable to many bone defects.26 Results from a number of different series have demonstrated good results of femoral revision with those implants that gain initial mechanical stability and long-term biologic fixation (by bone ingrowth) in the diaphyseal bone of the femur, which is usually well preserved (Fig. 21-9).27–30 Advantages of this philosophy include the relative simplicity of the techniques and the high potential for biologic fixation. Drawbacks include the risk of intraoperative fracture31 (Fig. 21-10) due to the tight mechanical pressfit required for success, difficulty of implant extraction after osteointegration, and potential for proximal bone stress shielding (Fig. 21-11).32 Patients with poor bone quality appear to be at highest risk for marked stress shielding. Large-diameter stiff implants probably increase the likelihood of stress shielding. In patients with very large canals and a limited remaining tube of diaphysis, higher failure rates with this method have been reported.33 These implants are discussed in more detail in Chapter 25.
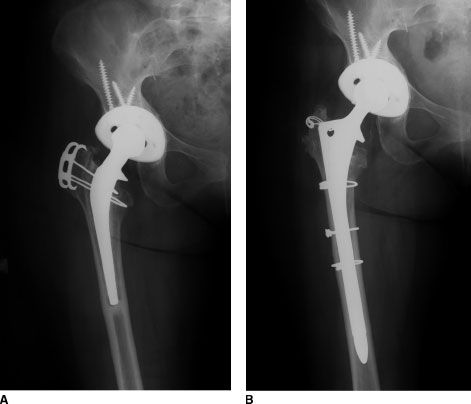
FIGURE 21-7. A: Radiograph of failed total hip arthroplasty. B: Radiograph after reconstruction with uncemented extensively porous-coated stem.
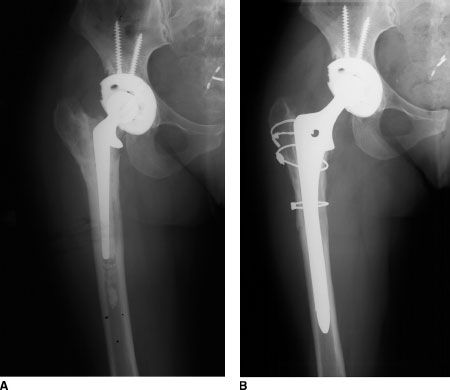
FIGURE 21-8. A: Radiograph of failed total hip arthroplasty. B: Radiograph after reconstruction with uncemented extensively porous-coated stem.
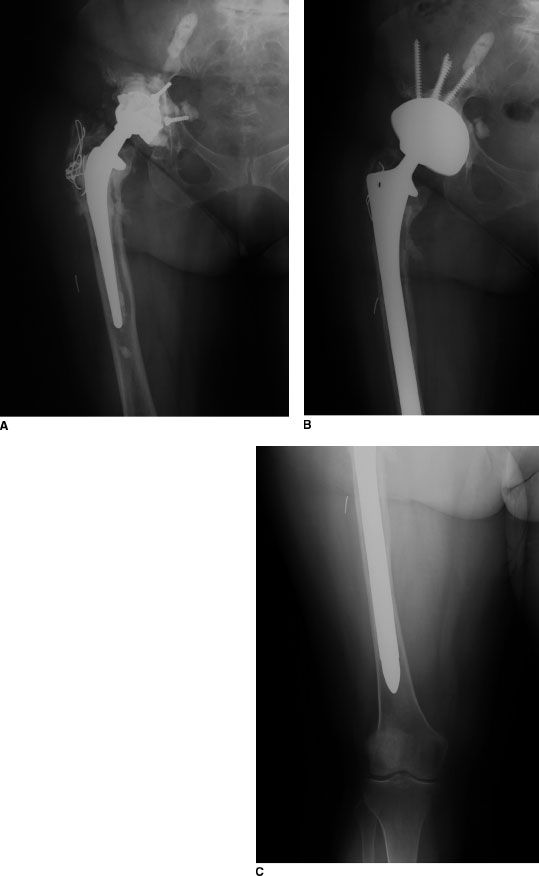
FIGURE 21-9. A: Radiograph of failed total hip arthroplasty. B,C: Radiograph after reconstruction with uncemented extensively porous-coated stem.
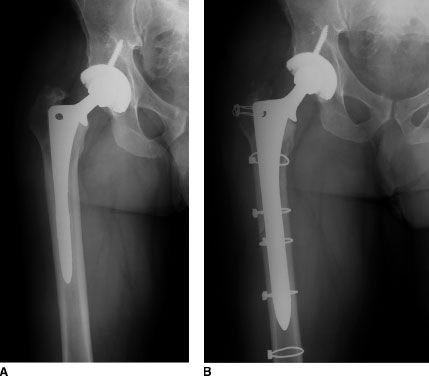
FIGURE 21-10. A: Radiograph of failed revision total hip arthroplasty. B: Postoperative radiograph after revision during which distal longitudinal intraoperative femur fracture was recognized and treated with cerclage cables
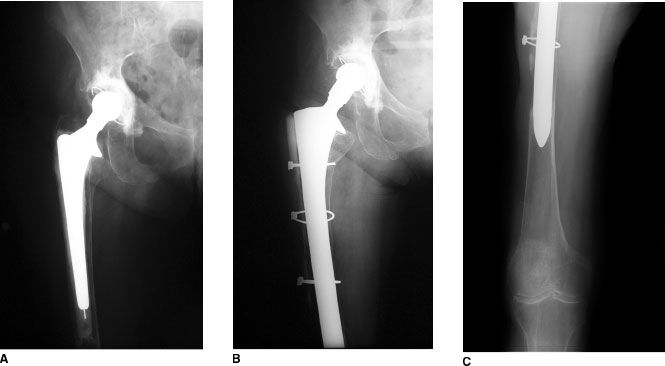
FIGURE 21-11. A: Radiograph of failed total hip arthroplasty. Note the poor bone quality and lack of trochanter. B,C: Radiograph 7 years after revision with long extensively coated stem. The stem is bone ingrown but there is severe stress shielding. This severity of stress shielding is uncommon.
Modular Fluted Tapered Implants
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


