Fig. 36.1
UNIC shoulder prosthesis system: one single range of humeral stems (cementless, cemented, trauma) fits all articular options (hemi, anatomic, reverse, CTA)
With regard to the fundamental principles of reverse shoulder prostheses, our prosthesis designers faced challenges of design optimization between the deltoid moment, the articular stability, the mechanical constraints of the glenoid base, and scapular notching. Optimal design rationalization depended upon consideration of some complex solutions, such as:
The mechanical constraints on the glenoid base are reduced increasingly as the center of articular rotation is medialized (shortening of the moment).
The optimization of the deltoid moment results from a compromise between the medialization of the humerus and its distalization. Pascal Boileau estimates an average medialization of 16 mm and an average distalization of 15 mm in a review of 45 Delta (Depuy, Warsaw, USA) prostheses evaluated in 2005 [1]. The Delta III prosthesis, as well as some other prostheses, reproduces an articular glenohumeral plan very horizontalized with regard to the anatomy. This favors the distalization of the humerus.
The articular stability is in direct relation with the tension of the deltoid. The prosthesis has to allow a fine-tuning of this tension intra-operatively, but if the tension of the deltoid is obtained by distalization of the humerus rather than by its lateralization, it can result in a partial de-cooptation between the humeral cup and the glenoid sphere, which generates instability during movements in external rotation.
The scapular notchings are inferred by a conflict between the most internal edge of the humeral cup and the subscapular pillar. The more the diameter of the humeral cup and the more it is horizontalized—which is in favor of the stability—and the more the humerus is distalized—which is in favor of the deltoid moment—then more contact may occur between the humeral cup and subscapular pillar.
Our challenge thus was to determine how to act on one or another of these variables without compromising the balance and the results thereafter.
Theoretical Basis for the Design Rationale of the UNIC Reverse Shoulder Prosthesis
The horizontalization at 155° of the articular plan of the humeral cup is a primary issue. This proposed angle relates to the articular stability in opposition to the vertical dislocating forces, but introduces problems during mobilization in adduction because of an asymmetric de-cooptation mechanism. The contact between the cup and the sphere transfers gradually from congruent to tangential. The cup positions between overriding below the subscapular pillar and point-contact de-cooptation, which results in transmission of perpendicular stresses to the glenoid fixation.
Added to this problem is the relative position of the cup in relationship to the humeral stem. The appreciation of this positioning is made complex by the diversity of the geometries of implants. It is about a combination of resection height with regard to the intra-medullary axis, its slope, and the position of the summit of this angle on the intra-medullary axis. In practice, humeral cups are more or less proximal, more or less tilted, and more or less medialized.
The designs specific to the reverse shoulders generally take into consideration the “necessity of incorporating the medial offset of the humeral head” as described by G. Walch in 1993 for the anatomic arthroplasty surgeries [2]. However in the case of a RTSA, the humerus which is medialized and distalized forces the humeral cup in a position that is increasingly medial.
When the distalization of the prosthetic center of rotation is obtained at the cost of a horizontalized and a medialized cup, the cup positions spontaneously over time under the glenoid sphere which poses 2 problems: a vicinity of contact between the edge of the humeral liner and the subscapular pillar, and a perpendicular stress on the glenoid base fixation in the first degrees of abduction.
On this basis of reasoning, our designers configured a slightly more proximal positioning (thus more lateral) of the cup with an articular angle corrected to a theoretical estimate between 138° and 145°. This should allow for:
Regaining humeral distalization value, while lateralizing the axis of the limb to the advantage of the muscular tension and of the intra-articular stability,
Offsetting the internal edge of the cup from impedance with the subscapular pillar,
Maintaining a congruency between the liner and the sphere at all degrees of mobility, and
Transmitting more compressive stresses to the glenoid fixation while decreasing perpendicular stresses.
Design Rationale of the Reverse Cup
The concept of a humeral “platform” system suitable with anatomic or reverse articular components involves that the angle, the level of humeral resection, and the mode of connection of the articular components are complimentary. The humeral resection angle is fixed “anatomically” at 132° and limited in thickness to the humeral head. The reverse humeral cup integrates an angular correction intended to horizontalize its articular plan. The correction angle is 8° and requires attention during implantation at the risk of excessively verticalizing the articular plan if the cup happens to be inverted.
Apart from this angular correction, there are no particular formulated criteria for the development of the humeral cup. However during the development of the anatomic version, a member of the design team suggested crossing two independent adjustment plans at 90° to solve the centering problem of the anatomic head without influencing the longitudinal axis. This idea consisted in crossing two crenelated racks in the sagittal and frontal planes, interconnected by a double-tapered modulus available in several angulations (Fig. 36.2). This system presents the advantage of managing the medial–lateral positioning of the head and its antero-posterior positioning in an independent way, and allows tuning of the angulation of the humeral head for a better adaptation to the anatomy while maintaining the oblong humeral head in its anatomic orientation. On the humeral stem side, this crenelated rack is oriented along the medial–lateral axis and from distal to proximal. The length and the crenels of the rack are identical for all the sizes of stems, and its calibration is indexed to the internal border of the stem.
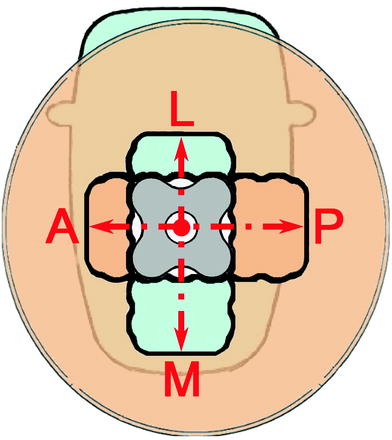
Fig. 36.2
90° crossing of 2 crenelated racks connected by a double-tapered modulus. The system allows for independent M/L and A/P positioning of the head on the cup
In theory, according to the position of the cup on the rack, it is possible to properly adjust the limb length (position at the top of the rack) or its lateralization (position at the bottom of the rack). Our design team intended for this adjustment to be used intra-operatively to tune and adapt the implant to the surgical situation while optimizing articular stability and mobility.
Related posts:
 Intact Rotator Cuff
Origins of Reverse Shoulder Arthroplasty and Common Misconceptions
1 History of Reverse Shoulder Arthroplasty
6 Preoperative Work-up and Surgical Approaches for Reverse Shoulder Arthroplasty
23 Debate: Patient-Specific Instrumentation Is Necessary versus It Is Not Necessary in All Cases
28 The Use of Convertible Glenoid Component Makes Revision to Reverse Total Shoulder Arthroplasty Easier
Intact Rotator Cuff
Origins of Reverse Shoulder Arthroplasty and Common Misconceptions
1 History of Reverse Shoulder Arthroplasty
6 Preoperative Work-up and Surgical Approaches for Reverse Shoulder Arthroplasty
23 Debate: Patient-Specific Instrumentation Is Necessary versus It Is Not Necessary in All Cases
28 The Use of Convertible Glenoid Component Makes Revision to Reverse Total Shoulder Arthroplasty Easier
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


