, George C. Babis2 and Kalliopi Lampropoulou-Adamidou3
(1)
Orthopaedic Department Medical School, National and Kapodistrian University, Athens, Greece
(2)
2nd Orthopaedic Department Medical School, National and Kapodistrian University Nea Ionia General Hospital “Konstantopoulion”, Athens, Greece
(3)
3rd Orthopaedic Department, National and Kapodistrian University KAT General Hospital, Athens, Greece
Abstract
The epidemiology, demographics and natural history of the three types of congenital hip disease in adults are presented. Dysplasia is the most common type of the disease, while low and high dislocations have almost the same incidence. The majority of patients with congenital hip disease are women. Knowledge of the natural history of congenital hip disease is essential for the understanding of the potential development and progress of its types.
4.1 Epidemiology and Demographics
The reported incidence of neonatal hip dislocation was found to be about 1–2 per 1,000 births [1], and this of neonatal hip instability is higher, between 1.6 and 28.5 per 1,000 [2]. Risk factors are family history, firstborn, breech position, possibly high birth weight and older maternal age as well as swaddling. The latter is considered that exerts unfavourable effect on the future course of an unstable hip [1]. It has been reported that usually instability is transient and resolves spontaneously in the first weeks of life [3].
The published epidemiological data regarding congenital hip disease (CHD) are heterogeneous, due to different diagnostic tools (e.g. physical examination, ultrasonography and plain radiographs), different population’s age, different ethnicities/races and geographic location, different observers and the rarity of the disease. Also there is difficulty in distinguishing the neonatal hip dysplasia from the hip instability, which resolves spontaneously. In a study from New Zealand, clinical examination of 20,657 newborns revealed that the 3.2 % were considered to have hip instability at birth. The half of these hips were stabilised completely within 5 days [4].
The incidence of CHD presents significant variability between and within racial groups and geographic locations. Caucasian infants demonstrate 42.2 ‰ (3.8–103 ‰) incidence at birth [1]. Particularly, Sweden has an incidence of 7.6 ‰ [5], England 66.0 ‰ [6], Greece 10.6 ‰ [7] and Italy 6.3 ‰ [8]. Turks, which are Indo-Mediterraneans, have 47.1 ‰ [9], and Africans, in many studies, 0 ‰ [10]. The prevalence is higher in Asians, as Japanese women have 116 ‰ and men 51 ‰ [11]. Differences may be found between residents of the same geographic area with different ethnicities, as the incidence of CHD of general Israeli population is 55 ‰ and that of Ethiopian Jews is much lower (12.4 ‰) [12].
In adults, most epidemiological studies of CHD are based on coincidental urograms or colon radiographs. Percentages vary in the literature depending on the criteria of assessment and the available data used in each study. In adults, the prevalence of CHD is reported to be between 4 and 10 %, which is much higher of that found in newborns may be due to many undiagnosed or subtle cases at birth [13]. The major concern is that CHD is a significant risk factor for the development of secondary osteoarthritis (OA). Radiographic evaluation of 468 patients (660 hips) with OA of the hip of our registry confirmed that 356 hips (54 %) had OA secondary to CHD, 272 hips (41 %) had idiopathic OA and in 74 hips (5 %), the cause of OA was uncertain (Fig. 4.1). In the majority of patients with CHD, both hips are involved. In our registry of the 231 patients with CHD, 125 had bilateral CHD, 17 had idiopathic OA of the contralateral hip and 89 patients had a normal contralateral hip [14].
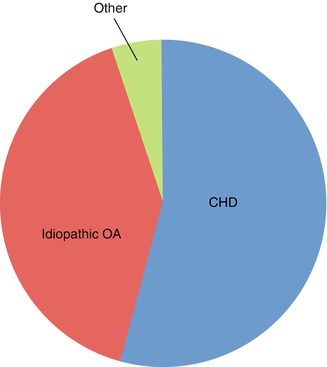
Fig. 4.1
Depiction of the proportion of different types of OA in 660 hips of our registry
Among the three types of the disease, dysplasia was found to be more common, while low and high dislocation were found to have similar incidence. Left and right hips were equally involved in dysplasia and low dislocation, while left-to-right hip ratio was approximately 2:1 in high dislocation. The great majority of patients with CHD (approximately 90 %) were women [14].
4.2 Natural History
Three radiographic types of CHD in infants have been recognised: (1) dysplasia, in which poor acetabular and femoral head development, with an intact Shenton’s line , is found, (2) subluxation, in which the Shenton’s line is broken, due to the proximal migration of the femoral head, without later overpassing the upper edge of the acetabulum and (3) complete dislocation , in which the femoral head is completely out of the acetabulum [15]. These three types correspond to dysplasia, low dislocation and high dislocation in adults (Table 4.1, Fig. 4.2)
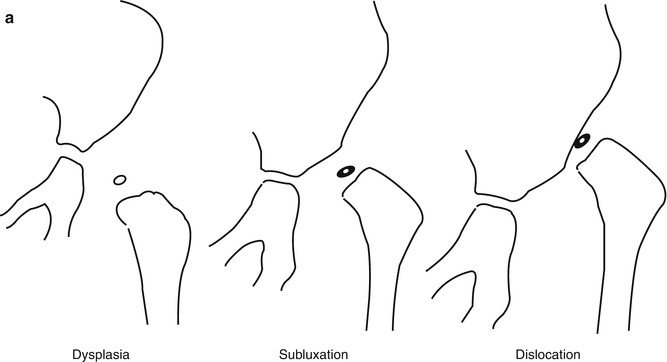
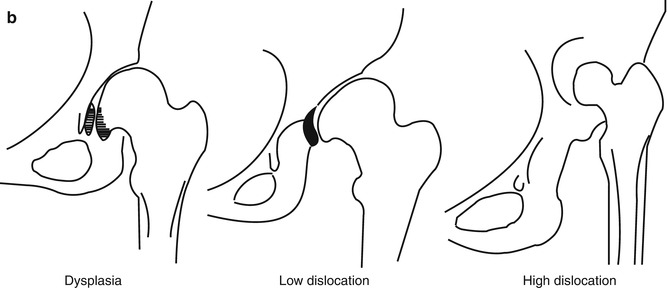
Table 4.1
Congenital hip disease in infants and in adults
Infants | Adults |
|---|---|
Dysplasia | Dysplasia |
Subluxation | Low dislocation |
Dislocation | High dislocation |
Fig. 4.2
The three types of the disease in infants (a) and in adults (b)
Early diagnosed dysplastic hips are treated successfully with the use for a few months of abduction devices (Figs. 4.3, 4.4 and 4.5). However, the majority of dysplastic hips remain undiagnosed. Diagnosis in these cases is established with the onset of early symptoms usually during the second or third decade of patient’s life or as incidental radiographic finding. Dysfunction, moderate pain and mild limp are the initial symptoms. The definition of a hip as dysplastic is of great importance. In a study, performed on 95 OA-free hips, we found that minor deviation of radiographic indices considered as normal should not characterise a hip as dysplastic and predict the development of OA [16]. The considered as normal values of the four more stated radiographic indices are presented in Fig. 4.6. Degenerative changes in a dysplastic hip develop progressively following biomechanical patterns (Fig. 4.7) [17–19]. The superolateral joint space gradually narrows and the femoral head becomes elliptical, due to the formation of marginal osteophytes .
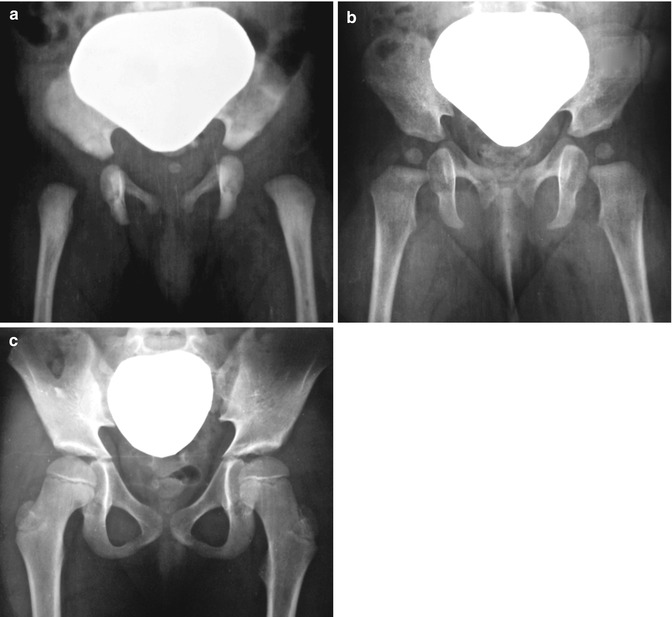
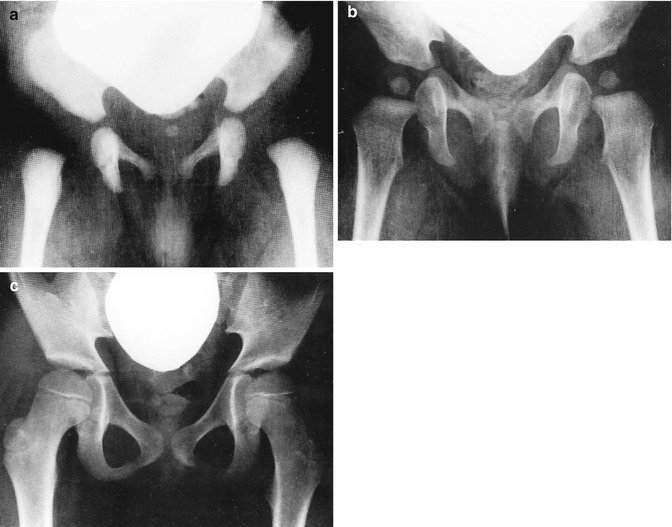
Fig. 4.3
The evolution of dysplastic hips early detected because of family history of CHD. (a) The infant’s pelvic radiograph 10 days after birth. The inclination of both acetabuli was considered as abnormal and an abduction pillow was applied. (b) At the age of 8 months, anteroposterior pelvis radiograph showed normal evolution of the hips and application of the pillow was discontinued. (c) Patient at the age of 9 with normal hips
Fig. 4.4




Female with bilateral dysplastic hips. The reason that radiograph was taken in this baby was that her mother was treated by us for bilateral CHD. (a) At the age of 3 months. Note the inclination of both acetabuli. An abduction pillow was applied. (b) At the age of 13 months, there is normal development of the femoral heads and acetabuli. (c) At the latest follow-up, at the age of 8
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
