88
Enchondroma
Kevin D. Plancher and Michael Bothwell
History and Clinical Presentation
A 22-year-old woman with no prior hand injury presents after feeling a snap in her left ring finger while playing volleyball. The patient reports pain and swelling. She also reports pain with motion of the finger.
Physical Examination
The finger is tender to palpation. Range of motion is limited due to pain.
Diagnostic Studies
On radiographs a pathologic fracture in the hand or digits is frequently noted. Plain x-rays are diagnostic and reveal a centrally located lesion with marked bone expansion (Fig. 88–1). Cortical thinning and calcifications may also be present. Computed tomography (CT) has proven to be a useful tool in diagnosing enchondromas because it may detect endosteal scalloping and reveal the amount of bone destruction.
Histologically, this cartilage lesion is lobular and may penetrate the surrounding marrow spaces. The cells are often surrounded by a well-defined area of a proteoglycan matrix and a narrow rim of bone (Fig. 88–2).

Figure 88–1. Radiographic finding of enchondroma of the proximal phalanx of the ring finger.
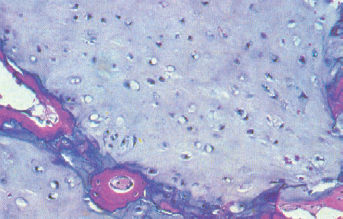
Figure 88–2. Histology of enchondroma showing cartilage lobular surrounded by narrow rim of bone.
Differential Diagnosis
Inclusion cyst
Fibrocystic defect of bone
Giant cell tumors
Aneurysmal bone cysts
Fracture
Enchondroma
Diagnosis
Enchondroma is the most predominant osseous tumor of the hand and is seen most frequently in the metacarpals and phalanges of the hand, but rarely affects the carpal bones, and accounts for approximately one fourth of all benign tumors. Enchondromas do not show a sex predilection, and can occur at any age, although most frequently they are seen in young adults. Most patients complain of pain in the fingers.
Surgical Management
The fracture was protected and allowed to heal in proper alignment. After the fracture had healed, the enchondroma was in its original state, as demonstrated by radiographs. The enchondroma was then excised by making a window in the cortex (Fig. 88–3). The contents, soft, blue, cartilaginous material, were carefully curetted. The cavity was then filled with cancellous bone (Fig. 88–4). The patient began early motion of the finger and returned for radiographs. No sign of the mass was seen.
Treatment consists of operative intervention when a fracture has occurred through the lesion. There is still a debate whether to treat the tumor and fracture simultaneously or wait until the fracture heals and perform surgery at a later date. Curettage and bone grafting is the preferred option. If useful function of the finger is lost, amputation may be necessary.





