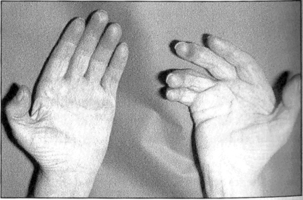
5.2 Dupuytren’s disease and other fibrocontractive disorders In an individual afflicted by Dupuytren’s disease, there is a usually a progressive decrease in their ability to carry out any tasks they could “imagine or desire” and they are brought to the point of severe frustration and annoyance as the disease progressively and irreversibly develops, as ultimately the result can be a permanent deformity of the hand, with fingers firmly lodged again the palm, incapable of performing their everyday normal functions (Pratt & Byrne 2009). This, it is fully accepted, is the most extreme form of the disease, but when such a state is reached and sometimes even in those people who are suffering the less severe forms of the condition, then the tasks of trying to carry out “anything which reason can imagine or desire” become clearly very difficult and, in the worst case, impossible. The condition gives rise to new connective tissue fibers and also new cells in a location where there should be no unnecessary connective tissue or additional cells. Biochemical studies have established that the newly formed collagen is a mixture of type III and type I, with collagen II being the predominant type associated with the nodules. The cells within the nodules have some of the functional characteristics of fibroblasts – synthesizing this new collagen – and ultrastructural similarities to some aspects of smooth muscle cells – giving rise to the contraction seen in the disease (Fig. 5.2.1).
Introduction
Palmar nodules
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


