Distal Radius and Carpal Fractures
CASE PRESENTATION
A 17-year-old male suffered a fall onto his extended wrist while playing basketball 2 months ago at boarding school. His wrist has hurt intermittently with sports, push-ups, and some activities of daily living with his wrist extended. He never sought medical attention while at school. He is home for the winter holidays, and his mother decided to bring him in for an evaluation. He has snuffbox, scaphoid tubercle, and thumb axial compression pain. His wrist extension is limited compared to the opposite side. His radiographs 2 months postinjury are seen in Figure 34-1A. His computated tomography (CT) scan is seen in Figure 34-1B.
CLINICAL QUESTIONS
Do nondisplaced distal radial metaphyseal buckle fractures require cast treatment?
Is there an outcome difference between long-arm and short-arm cast immobilization for distal radius fractures treated with CR?
How much and over what time can a distal radius fracture remodel?
What are the indications for CRPP of distal radius fractures?
What are the indications for ORIF of distal radius fractures?
When should ulnar styloid fractures be acutely fixed?
What is the risk of growth arrest in a distal radius physeal fracture?
What are the indications for an ulnar shortening osteotomy?
Which scaphoid fractures should be treated with cast immobilization in children and adolescents?
What are the indications for percutaneous scaphoid screw fixation?
Should every scaphoid nonunion in the pediatric age group be treated surgically?
What is the surgical approach for an acute transscaphoid perilunate dislocation?
THE FUNDAMENTALS
Etiology and Epidemiology
The distal radius (in isolation or with a distal ulna fracture) is the most common site of a pediatric fracture.1, 2, 3 and 4 Distal radius fractures occur most commonly in adolescent patients, almost exclusively secondary to a fall. A fracture during a sporting event is a common occurrence, in particular skateboarding, snowboarding, and soccer goalkeeping, among others.5, 6 and 7 Protective wrist guards are of benefit in reducing fracture risk in these sports.8 Children with obesity and poor bone mineralization are at more risk for a fracture with a routine fall.9, 10, 11 and 12 Repetitive stress loading of the wrist, such as with gymnastics, can lead to a distal radial physeal stress fracture (see Chapter 39).13, 14, 15 and 16 Triangular fibrocartilage complex (TFCC) tears (see Chapter 42) are more common with positive ulnar variance, and Kienbock disease (avascular necrosis [AVN] of the lunate) (Figure 34-2) is more common with negative ulnar variance.
Clinical Evaluation
Children and adolescents with a distal radius fracture will present with localized pain and restricted motion. Nondisplaced fractures in the young may have minimal pain or restrictions due to periosteal stabilization. Displaced fractures of the distal radius and ulna will have obvious deformity. With markedly displaced fractures, neurovascular (NV) compromise can occur. Open fractures do occur and are more at risk for NV impairment.
Distal forearm fractures are classified radiographically by location of fracture (metaphyseal or physeal), direction (volar or dorsal) and degree of displacement, and bone involved (radius, ulna, or both). Metaphyseal fractures are further defined as torus/buckle (one cortex and therefore stable), both cortices (potentially unstable), and complete, displaced fractures. Most distal forearm fractures extend due to the fall on an outstretched wrist mechanism of injury. A variant is the pediatric Galeazzi fracture dislocation: a displaced distal radial metaphyseal fracture with either a distal ulnar physeal fracture or distal radioulnar joint (DRUJ) dislocation. Transphyseal fractures are less common than metaphyseal fractures and are defined by standard Salter-Harris classification.17 Salter-Harris type II, followed by Salter-Harris type I, injuries are the most common displaced distal radial physeal fractures. Intra-articular fractures are uncommon with an open physis (Salter-Harris type III) but are more and more common with skeletally mature adolescents during their highly competitive sports participation. Classification of intra-articular distal radius fractures is similar to adults. The use of CT scans is necessary to define displacement, number of fracture fragments, and operative indications.
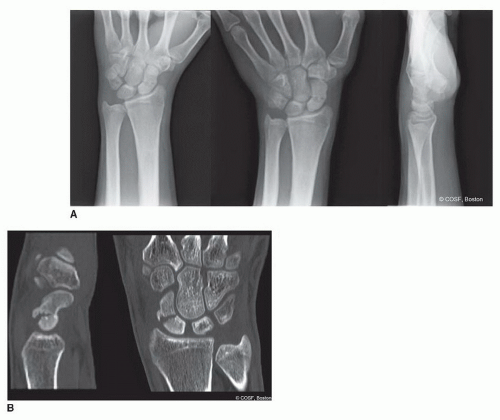 FIGURE 34-1 A: Radiographs of mildly displaced scaphoid fracture that occurred 2 months before. B: CT scan confirms mild humpback deformity, fracture with minor cystic changes. |
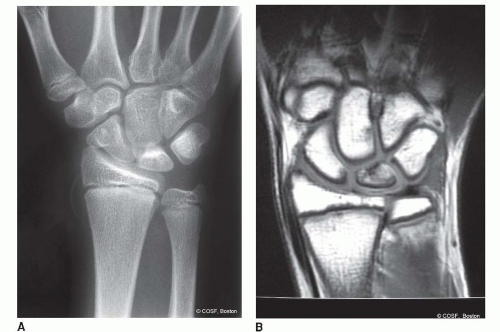 FIGURE 34-2 A: Mild Kienbock disease anteroposterior (AP) radiograph and (B) confirmed on magnetic resonance imaging (MRI) scan. |
Scaphoid fractures are more subtle than distal radius and ulna fractures by history and exam.18,19 Snuffbox tenderness, scaphoid tubercle tenderness, and axial compression of the thumb are all sensitive physical exam findings for an acute scaphoid fracture or chronic nonunion, but axial compression is the most specific. Plain radiographs need to include a 30-degree ulnar deviation AP view (scaphoid view). Scaphoid fractures are defined by location of the fracture (waist, proximal, or distal pole) and displacement (nondisplaced, <2 mm, >2 mm). Proximal pole fractures have the highest risk of AVN. The use of CT scans is often necessary to define operative indications (displaced fractures >2 mm) but need to be taken in the longitudinal plane of the scaphoid to be accurate.20,21 The use of MRI scans is appropriate for patients with snuffbox tenderness, scaphoid tubercle tenderness, and/or thumb axial compression pain but normal plain radiographs22, 23, 24 and 25 (Figure 34-3). Scaphoid nonunions usually present long after the fracture and often with lack of treatment since the time of injury. The pain is usually mild, worse with wrist extension and axial loading activities, and often not debilitating. There is generally limited wrist extension and scaphoid-specific pain on physical exam. X-rays will reveal the nonunion and possible AVN of the proximal pole with scaphoid collapse (dorsal intercalary segment instability [DISI] pattern with the distal pole of the scaphoid flexed and lunate extended on the lateral radiographic image).
 FIGURE 34-3 A: Original radiographs of the scaphoid were interpreted as negative for fracture. B: MRI 3 weeks later reveals scaphoid fracture. C: Percutaneous scaphoid screw fixation was the treatment of choice for this patient with radiographic healing noted. |
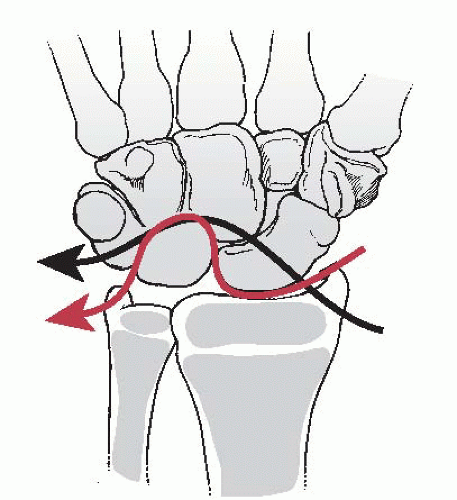 FIGURE 34-4 Disruption pattern of a trans-scaphoid perilunate dislocation (black line) or pure perilunate dislocation (red line) noted by illustration. (From Beaty JH, Kasser JR. Rockwood & Wilkins Fractures in Children. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.) |
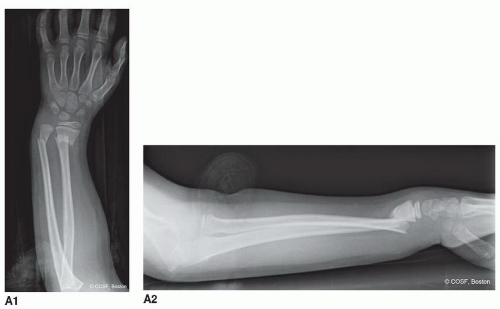 FIGURE 34-5 A: Injury films of displaced distal radius and ulna fractures. |
Trans-scaphoid perilunate dissociations are the most common type of acute perilunate carpal dislocations. These dislocations are rare and secondary to a high-velocity injury in extreme wrist dorsiflexion. An acute median neuropathy is common with a complete perilunate dislocation. There is usually marked swelling, deformity, and pain. Inexplicably, some of these patients present days after injury, which heightens the risk of AVN of the scaphoid proximal pole and/or dislocated lunate. The force of a perilunate dislocation starts radially either through the scaphoid as a fracture or through the scapholunate ligament; it then extends between the lunate and capitate dissociating the proximal and distal carpal rows; and finally it returns to the ulnocarpal joint in a clockwise fashion through the lunotriquetral joint (Figure 34-4). In a complete injury, the lunate usually ends up volar in the carpal canal, and the radius and capitate become colinear.
Surgical Indications
All displaced fractures and dislocations of the distal forearm and wrist require treatment. The major defining factors for treatment type closed reduction (CR), closed reduction percutaneous pinning (CRPP), or open reduction and internal fixation (ORIF) for distal radius and/or ulna fractures is the age of the patient, degree and direction of displacement, and any articular involvement. If the child is young (>2 years of growth remaining), the fracture is extra-articular and displaced in the plane of motion of the joint and has <20 degrees of malangulation without malrotation, then the bone will eventually remodel. Using CR and cast treatment is appropriate with close follow-up.26, 27 and 28 Some fractures treated with CR will redisplace and require either repeat CR or CRPP (Figure 34-5).
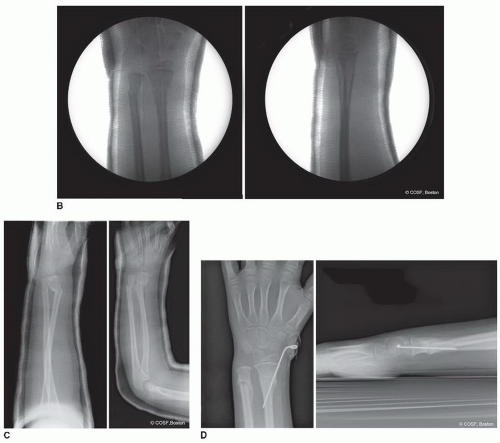 FIGURE 34-5 (continued) B: Conscious sedation reduction in emergency department is near-anatomic reduction. C: Loss of reduction in cast is noted on radiographs 13 days later. D: CRPP to anatomic alignment and healed fractures just before pin removal in office. |
In skeletally mature adolescent patients, CRPP or ORIF is indicated for displaced fractures to restore radial inclination, physiologic ulnar variance, and DRUJ alignment. All displaced intra-articular fractures require anatomic reduction and rigid fixation.
Displaced scaphoid fractures29 and scaphoid nonunions require anatomic reduction and fixation. Nondisplaced, acute fractures without bone loss, and proximal pole scaphoid fractures, can be treated with percutaneous screw fixation.30 Acute fractures and chronic nonunions with bone loss require ORIF with bone graft to restore carpal alignment and expedite healing.31, 32, 33 and 34
All displaced perilunate dislocations require operative reduction and stabilization. Although there is debate about the method of treatment (CRPP or ORIF) and surgical approach with open reduction (volar, dorsal, or combined), there is no debate about the need for reduction and stabilization for the best results.
SURGICAL PROCEDURES
• Closed Treatment of Stable Fractures
Nondisplaced unicortical fractures of the distal radius and/or ulna metaphysis are stable injuries. A removable Velcro splint, posterior plaster or fiberglass splint, or bivalve cast immobilization have all been successful forms of treatment.35,36 There is some evidence that these patients may not need to return for follow-up appointments and still have uncomplicated outcomes.37 The only potential
problem is mistaking a bicortical, unstable fracture for a stable injury. The bicortical fractures may have been more displaced at the time of injury and can redisplace in nonrestrictive immobilization. Nondisplaced metaphyseal distal radius and/or ulna fractures are usually clinically healed by 3 to 4 weeks, at which time the immobilization can either be discontinued at home by patient and family or in the office by medical personnel. Repeat radiographs are often not obtained.
problem is mistaking a bicortical, unstable fracture for a stable injury. The bicortical fractures may have been more displaced at the time of injury and can redisplace in nonrestrictive immobilization. Nondisplaced metaphyseal distal radius and/or ulna fractures are usually clinically healed by 3 to 4 weeks, at which time the immobilization can either be discontinued at home by patient and family or in the office by medical personnel. Repeat radiographs are often not obtained.
• CR of Distal Radius and Ulna Fractures
Displaced distal radius and/or ulna fractures usually require reduction to realign the bones and joints and lessen the risk of further displacement over the next 3 weeks of healing. The reductions are generally performed in the emergency room with conscious sedation.
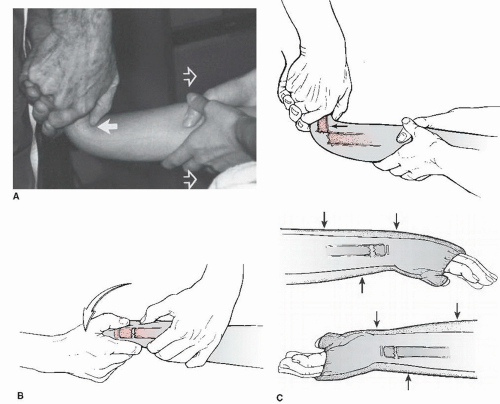 FIGURE 34-6 Illustrations of CR of distal radial metaphyseal fracture note the accentuation of the deformity (A) followed by reduction of the fracture by bringing the dorsal, distal fragment over the top of the volar, proximal fragment. B, C: Three-point molding is performed with cast application. (From Beaty JH, Kasser JR. Rockwood & Wilkins Fractures in Children. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.) |
Conscious sedation is performed by the emergency room attending staff with in-hospital anesthesia attending as backup. Once the patient is adequately sedated, the CR is achieved in a series of steps. For metaphyseal fractures with bayonet apposition, the deformity is initially accentuated (Figure 34-6A). The degree of deformity accentuation needed to unhinge a bayonet apposition fracture can be extreme, to the point of instilling nausea in the observing health care personnel. Once the fracture is unhinged and the dorsal periosteum is relaxed, the fracture fragment is “walked” distally with the extension deformity maintained. This maneuver will get the fracture out to length, but it takes very strong intrinsics and thumbs for most fractures. Many fall short with these first two maneuvers. Then the distal fracture fragment is reduced onto the proximal fragment metaphysis (Figure 34-6B) with dorsal to volar thumb pressure. Complete reduction may
take several back and forth maneuvers until the fracture is anatomic. Anything less than anatomic will have a higher risk of redisplacement over the next 3 weeks. Anatomic reduction can be felt by dorsal bony alignment, seen by loss of obvious deformity, and confirmed by fluoroscopy. Following anatomic reduction, the choice is well-molded cast immobilization or CRPP. Irreducible fractures require an open reduction by volar approach to extract interposed periosteum and/or pronator quadratus (PQ).38, 39 and 40
take several back and forth maneuvers until the fracture is anatomic. Anything less than anatomic will have a higher risk of redisplacement over the next 3 weeks. Anatomic reduction can be felt by dorsal bony alignment, seen by loss of obvious deformity, and confirmed by fluoroscopy. Following anatomic reduction, the choice is well-molded cast immobilization or CRPP. Irreducible fractures require an open reduction by volar approach to extract interposed periosteum and/or pronator quadratus (PQ).38, 39 and 40
Displaced physeal fractures require a gentler reduction. This can usually be performed with finger trap distraction and dorsal to volar finger reduction (Figure 34-7). The reduction is again performed under conscious sedation. Avoiding additional injury to the distal radius physis with reduction is imperative. This is usually not a difficult reduction. The reduction can also be done under hematoma block but does require a noncombative patient to prevent shear and compression stress injury to the physis. Anatomic reduction is confirmed by fluoroscopic images.
In both metaphyseal and physeal fractures, the dorsal periosteum acts as a tension band in helping maintain reduction. The wrist is positioned in slight (∽20 degrees) palmar flexion to provide dorsal periosteal tension. Cast padding and molding are key to providing external support for maintaining reduction. A dorsal mold directly over the fracture and a more proximal volar mold provide three-point fixation (Figure 34-6C). The dorsal mold cannot be too distal, or it will lead to venous congestion due to outflow obstruction on the dorsum of the hand. A straight ulna border and anatomic radial bow mold of the forearm are required. The results of long-arm and short-arm cast immobilization are equivalent,26,28 including prospective randomized studies.41,42 The most important factor is the quality, not the length, of the cast. The quality of the cast molding can be measured by the cast index, which is the sagittal diameter divided by the coronal diameter at the fracture site. A value of 0.7 or less defines a well-molded cast and carries less risk of loss of reduction (Figure 34-8A).
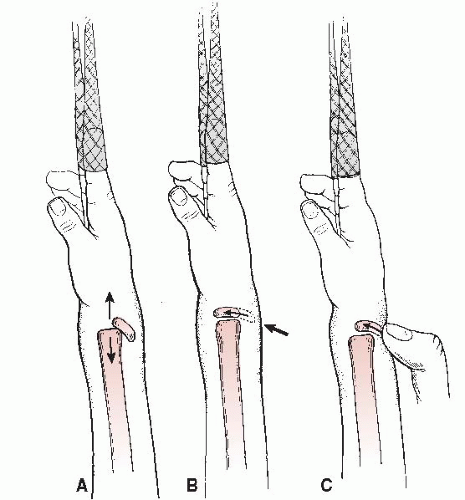 FIGURE 34-7 Illustration of distal radial physeal fracture reduction. Longitudinal traction (A) is followed by gentle dorsal-to-volar pressure on the distal epiphysis (B), usually preformed by the surgeon’s thumb (C). The reduction should be atraumatic to lessen the risk of growth arrest. Finger trap distraction and stabilization with a few pounds can help. (From Beaty JH, Kasser JR. Rockwood & Wilkins Fractures in Children. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.) |
Even with acceptable reductions and casts, there is a high rate of loss of reduction in distal radial metaphyseal fractures.43, 44, 45, 46, 47, 48 and 49 On average, the incidence of loss of reduction is 20% to 30%. Higher rates of fracture instability occur with isolated distal radial metaphyseal fractures,49 incomplete fracture reduction,44,45 and initial displacement >30 degrees, and the highest rates occur with complete displacement.50 The decision for the surgeon then is to allow the fracture to remodel; do a repeat CR and new cast application; or perform a CRPP. Ultimately, the choice among these options is dependent on the age of patient; degree of deformity; amount of fracture healing; and patient, parent, and surgeon preferences. Physeal fractures will remodel remarkably and are at risk for growth arrest if a repeat reduction is performed after 5 days from injury.51
▪ CRPP of Distal Radius Fractures
Due to the high rate of loss of reduction for distal radius metaphyseal fractures treated with CR cast immobilization, many centers perform CRPP as the primary approach for the fractures with complete displacement.52 Evidence by prospective study of distal radial metaphyseal fractures47,48 reveals that the results of CRPP and CR cast immobilization are equivalent at 2 years postinjury if (1) there is sufficient growth remaining for remodeling and (2) repeat reductions are performed when the fracture redisplaces in a cast. The surgeon, patient, and family can choose what is the best treatment for the patient (i.e., there is clinical equipoise). In older patients, there is not sufficient time for remodeling, so CRPP or ORIF is indicated in the skeletally mature or near skeletally mature patient with an unstable, displaced fracture (Figure 34-9).
In addition, distal radial physeal fractures with median neuropathy are candidates for CRPP to avoid NV compromise and/or unacceptable loss of reduction.53,54 Loss of reduction after initial CR cast immobilization of metaphyseal fractures can be treated with CRPP, but be careful about late reduction (more than 5 days postfracture) in physeal fractures due to risk of growth arrest. Finally, open fractures are candidates for CRPP, external fixation, or ORIF after operative washout of the contaminated bone and soft tissues.
 FIGURE 34-8 A: Markedly displaced distal radial physeal fracture treated with CR cast immobilization with excessive wrist flexion mold on lateral radiograph. B: CR of radius and ulna metaphyseal fractures with a poor cast index noted. The obvious loss of reduction is evident. |
The technique for the CR in the operating room under general anesthesia is the same as described by CR under conscious sedation in the emergency room. Once the fracture is aligned in the AP and lateral planes, sterile prepping and draping are performed. The arm is abducted onto a fluoroscopic arm table. Confirmation of the anatomic reduction on the fluoroscopic images is again obtained prior to pinning. Single or double pin techniques are used depending on the age of the patient and stability of the fracture. Blind pinning is avoided to prevent injury to the radial sensory nerve and/or extensor tendons. The first, and sometimes only, pin is placed obliquely from distal to proximal and radial to ulnar. Outlining the desired trajectory of the pin with a skin marker is helpful. A small incision is made distal to the radial styloid if the epiphysis is the entry site (distal physeal fractures and metaphyseal fractures
with a short distal metaphyseal segment). The incision is more proximal with a larger distal metaphyseal segment, so the pin can avoid the physis and pass exclusively in the metaphysis. Skin and subcutaneous dissection down to the bone is performed, and retractors are placed to protect the neighboring extensor tendons and radial sensory nerve. The pin is placed against the bone to match the planned trajectory marked on the skin. Fluoroscopic images are used to confirm the pin entry site, projected path, and to avoid false entry into the joint or surrounding important soft tissues. The pin is passed on oscillation with power to prevent entanglement of the soft tissues on the pin. The proximal ulnar cortex is penetrated proximal to the fracture site. The stability of the fracture is tested manually and with fluoroscopy. If the single pin is sufficient, then the CRPP is complete. If there are instability concerns, then a second parallel radial pin or a crossed pin is placed.
with a short distal metaphyseal segment). The incision is more proximal with a larger distal metaphyseal segment, so the pin can avoid the physis and pass exclusively in the metaphysis. Skin and subcutaneous dissection down to the bone is performed, and retractors are placed to protect the neighboring extensor tendons and radial sensory nerve. The pin is placed against the bone to match the planned trajectory marked on the skin. Fluoroscopic images are used to confirm the pin entry site, projected path, and to avoid false entry into the joint or surrounding important soft tissues. The pin is passed on oscillation with power to prevent entanglement of the soft tissues on the pin. The proximal ulnar cortex is penetrated proximal to the fracture site. The stability of the fracture is tested manually and with fluoroscopy. If the single pin is sufficient, then the CRPP is complete. If there are instability concerns, then a second parallel radial pin or a crossed pin is placed.
 FIGURE 34-9 A: Injury films reveal markedly displaced distal radial physeal and ulnar metaphyseal fractures. B: The radial physeal fracture was treated with CRPP and the ulna fracture with CR. C: Healed fractures at 2 months post-CRPP. Epiphyseal and metaphyseal pin tracks still evident, but no physeal arrest is present. |
An additional crossed pin may be placed from distal ulnar to proximal radial with the entry point between the fourth (extensor digitorum communis) and fifth (extensor digiti quinti) dorsal wrist compartments. The pin(s) is(are) left out of the skin, bent and cut, and dressed sterilely in a bulking fashion to prevent irritation, infection, or migration (Figure 34-10). Even some intra-articular fractures can be treated with CRPP (Figure 34-11).
▪ ORIF of Distal Radius Fractures
If winning isn’t everything, why do they keep score?
—Vince Lombardi
There are many different techniques for ORIF of an adolescent distal radial fracture. Volar and dorsal plating; locked, neutralization, and compression plating;
segmental fixation systems; and pin fixation have all been used successfully.55,56
segmental fixation systems; and pin fixation have all been used successfully.55,56
 FIGURE 34-10 Small incision noted with pins left out of skin for removal at 4 weeks. |
The choice of surgical approach and instrumentation is often fracture and patient specific (Figure 34-12). The goals are the same regardless of implant choice: anatomic, stable reduction of both the extra-articular and intra-articular fracture fragments that allows for full rehabilitation. That said, like the adult, the present volar distal radius locked, segmental fixation systems are effective for the adolescent displaced, unstable fracture that requires ORIF (Figure 34-13).
A volar approach to the distal radius is used.57,58 The flexor carpi radialis (FCR) tendon sheath is incised and the radial artery protected. The FCR tendon is mobilized. The digital flexors are swept ulnarly off the PQ. A moist sponge followed by a deep retractor is very effective. Crossing vascular channels are cauterized. The PQ is elevated off the radius with a deep linear incision to bone. If there is intra-articular involvement, the pronator is elevated with an upsidedown “L” incision all the way to the ulnar side of the radius. Subperiosteal retractors are placed radially and ulnarly after full subperiosteal exposure is performed of the bone and fracture site. This approach and technique are now commonplace for the modern-day orthopaedic trainee, as so many of the adult distal radius fractures are now plated volarly.
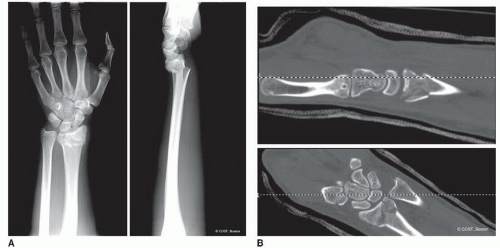 FIGURE 34-11 A: Injury films of displaced metaphyseal fracture with intra-articular extension. B: CT images of articular alignment. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


