Macrodactyly
CASE PRESENTATION
A 3-month-old female infant presents with an enlarged middle finger. There are no other associated systemic or musculoskeletal malformations. There is no family history of congenital differences and, in particular, of macrodactyly, limb hypertrophy, or neurofibromatosis. At this stage, the middle finger is already the length of the mother’s middle finger but wider. There is limited active motion present (Figure 7-1).
CLINICAL QUESTIONS
What causes digital and limb enlargement?
Is macrodactyly a genetic condition?
Are there associated malformations with digital or limb hypertrophy?
What is the evaluation of a child with macrodactyly or limb hypertrophy?
How is the clinical course monitored?
What are the surgical indications?
Which procedures are performed at which time?
What are the expected outcomes from natural history and/or surgery?
THE FUNDAMENTALS
You and I do not see things as they are. We see things as we are.
—Herb Cohen
Unfortunately, people continue to expect other people to fit in a perceived social norm. This is particularly true of the appearance of the hands and upper limbs. Digital enlargement or entire limb overgrowth, if profound or progressive, can be a psychosocial issue for affected children, their parents, and families. Even the pseudoscientific, descriptive term “gigantism” evokes perceived horror or a circusfreak quality for macrodactyly and limb overgrowth. Such stigma is unfair and detrimental to these children.
Enlargement of a limb does not necessarily make it less functional. If the motion and sensibility are normal, then the superhero-appearing limb functions quite well. However, if the enlarged digits or limbs are stiff, relatively insensate, painful, or weak, then function is impaired.
Etiology and Epidemiology
Increased vascular or neural supply will result in increased growth of all tissues (skin and soft tissues, muscles, and bones). Macrodactyly and limb hypertrophy are thus seen with lipofibrohamartomatous peripheral nerves (involving the median more commonly than ulnar nerves) and neurofibromatosis; vascular enlargement with arteriovenous fistulas, vascular malformations, and Klippel-Trenaunay syndrome; and lymphatic malformations. Increased bone and cartilage growth will result in macrodactyly, such as is seen with osteochondromatosis and Ollier enchondromatosis (see Chapters 47 and 49).1, 2, 3 and 4 Hemihypertrophy is a regional form of enlargement that can include part or all of one limb or the entire half of the body including the face. Hemihypertrophy can be associated with Wilms tumor. Enlargement can be due to congenital muscular hyperplasia of a limb.5 Limb hypertrophy can also be seen with more generalized syndromes such as Proteus or CLOVES.6, 7 and 8 Aside from neurofibromatosis, which has an autosomal dominant inheritance, all of these conditions are sporadic and rare. Macrodactyly due to lipofibromatosis of the nerve is rare in all races but less common in non-Caucasians. Blacks have more macrodactyly of the foot than of the hand.9
Clinical Evaluation
The principles of clinical evaluation involve defining (1) the form of macrodactyly or limb hypertrophy, (2) whether the postnatal growth is proportional or progressive, and (3) the width and length of the affected part compared to expected adult growth. These days, the diagnosis is often made in utero by ultrasound.10 Otherwise, in most cases, it is obvious at birth. Serial exams with exact length and girth measurements are recorded yearly from diagnosis. Plain radiographs are obtained to assess osseous deformity,
length of each bone, and physeal maturity compared to the opposite side. The use of magnetic resonance imaging (MRI) and computed tomography scans11, 12 and 13 provides definitive diagnosis by assessing fatty infiltration of lipofibromatous peripheral nerves, vascular anomalies, congenital muscular hyperplasia or anomalous muscles, and lymphatic malformations. With hemihypertrophy, a screening ultrasound is obtained for Wilms tumor. Electrodiagnostic studies are more sensitive than clinical exam in children for compressive neuropathy, a common complication of macrodactyly and limb hypertrophy.14,15
length of each bone, and physeal maturity compared to the opposite side. The use of magnetic resonance imaging (MRI) and computed tomography scans11, 12 and 13 provides definitive diagnosis by assessing fatty infiltration of lipofibromatous peripheral nerves, vascular anomalies, congenital muscular hyperplasia or anomalous muscles, and lymphatic malformations. With hemihypertrophy, a screening ultrasound is obtained for Wilms tumor. Electrodiagnostic studies are more sensitive than clinical exam in children for compressive neuropathy, a common complication of macrodactyly and limb hypertrophy.14,15
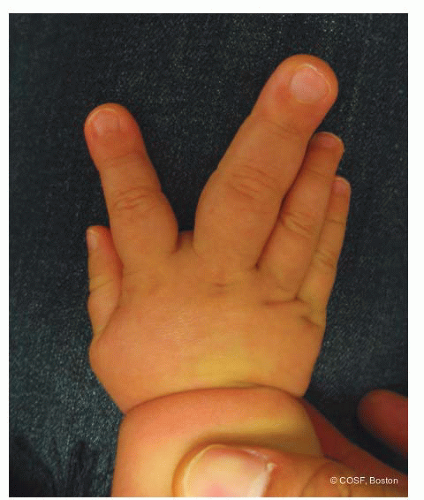 FIGURE 7-1 Macrodactyly of both the long and, less so, the index finger with divergence of the digits. An MRI of this patient revealed lipofibromatosis of the median nerve at the wrist extending distally to the common digital nerve and proper digital nerves of the index and long fingers. |
Flatt classified macrodactyly as: Type I is lipofibromatosis, type II is neurofibromatosis, type III is polyostotic, and type IV is hemihypertrophy. Lipofibromatosis has also been named lipofibroma hamartomatosis, macrodystrophia lipomatosa, and macrodactylia fibrolipomatosis, among others. The name signifies digital enlargement due to fat and fibrous infiltration in a peripheral nerve distribution, much more commonly in the median than the ulnar nerve (Figure 7-1).16,17 The index finger is most commonly involved, often in conjunction with the long finger or thumb. The dilation of the nerve often starts in the distal forearm and extends through the carpal canal and common digital nerve out to the proper digital nerve. The involved nerve has fatty infiltration and fibrosis. The bone often has altered architecture by biopsy with wide medullary canals and distorted trabeculae.18 The subcutaneous tissue is fibrotic. The skin is expansile with volar greater than dorsal, and distal greater than proximal, enlargement of skin and subcutaneous tissues.
Multiple digital involvement is more frequent than single digit. Unilateral hand involvement is most common. Syndactyly occurs in about 10% of cases. Asymmetric growth of each involved digit with angular and rotational malalignment is common and corresponds to the degree of proper digital nerve lipofibromatosis. The involved digit(s) often hyperextend and radially deviate due to more palmar and ulnar involvement. Flatt called these “banana fingers.” The growth can be progressive or proportional. With progressive enlargement, digital motion and function diminishes.
Sensibility by two-point discrimination and light touch measurements are, surprisingly, usually normal. However, compressive neuropathy can occur with loss of sensibility and motor function over time. This is usually due to a carpal tunnel syndrome14,15 but also has been described with lipofibromatosis of the ulnar nerve and cubital tunnel compression.19 Electrodiagnostic studies are often required due to limits of history and physical exam for carpal or cubital tunnel syndrome diagnosis in these children. There are children with lipofibromatosis of the median nerve who present with only a palpable mass in the distal forearm without macrodactyly. MRI and electromyography and nerve conduction velocity (EMG/NCV) studies are necessary for diagnosis. These lesions are usually monitored over time when the nerve is functioning normally since it is not a neoplasia. Neural decompression and carpal release are indicated if weakness and loss of sensibility develop.
Flatt’s other types of macrodactyly include neurofibromatosis, hemihypertrophy, and polyostotic forms. A syndromic class should be included with Proteus, CLOVES, and Klippel-Trenaunay syndromes, among others. In addition, congenital unilateral muscular hyperplasia is seen separate from hemihypertrophy. Vascular and lymphatic malformations will result in limb and/or digital enlargement. With all digits involved, upper limb and even truncal involvement, these conditions are more likely. MRI scan is used to define pathoanatomy and aid in diagnosis and treatment. Genetics consultation and multidisciplinary clinic evaluation and care are important in these situations.
Surgical Indications
The presence of macrodactyly or limb hypertrophy alone is not an indication for surgery. There is wide variation in clinical presentation. Some minor increases in size can be near normal in appearance and function. Alternatively, there are many instances of limb and/or digital hypertrophy that cannot be resolved or “normalized” even by surgical intervention. Often, care for these children is a case of managing expectations.
In the cases of lipofibromatosis of a major peripheral nerve, progressive deformity and loss of function are
indications for surgical treatment. Options include (1) soft tissue debulking, (2) appropriately timed physeal arrests, (3) digital realignment (Figure 7-2




indications for surgical treatment. Options include (1) soft tissue debulking, (2) appropriately timed physeal arrests, (3) digital realignment (Figure 7-2
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
